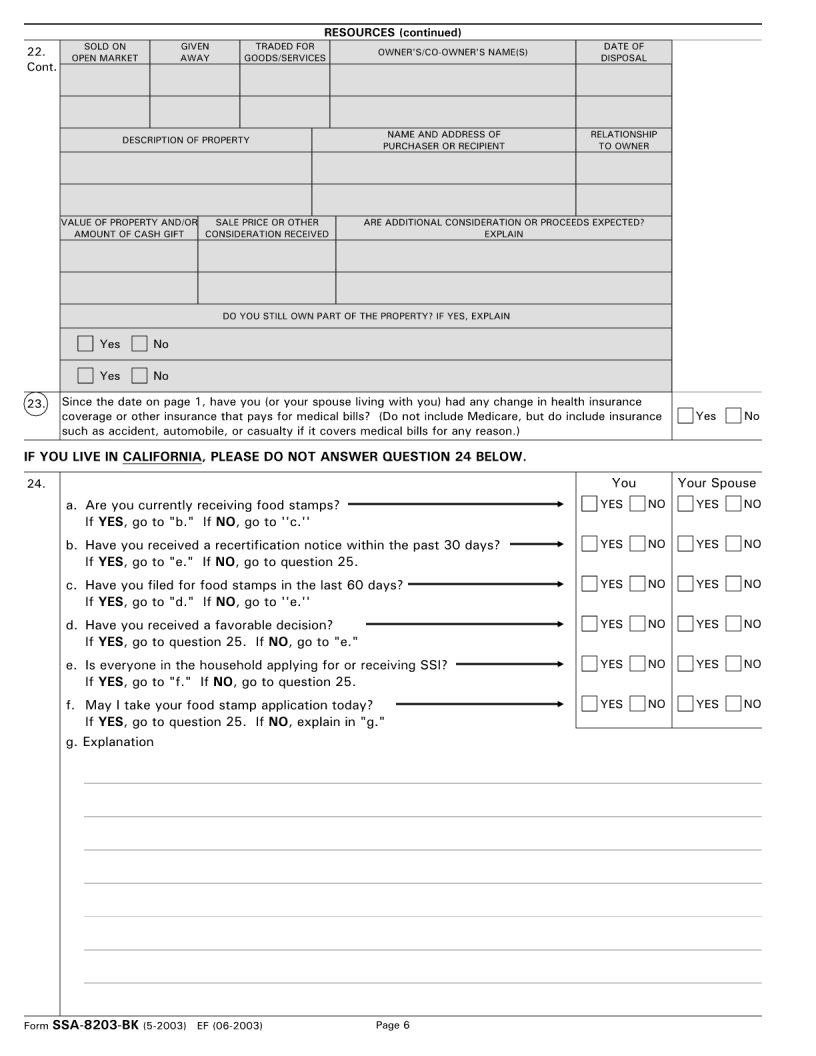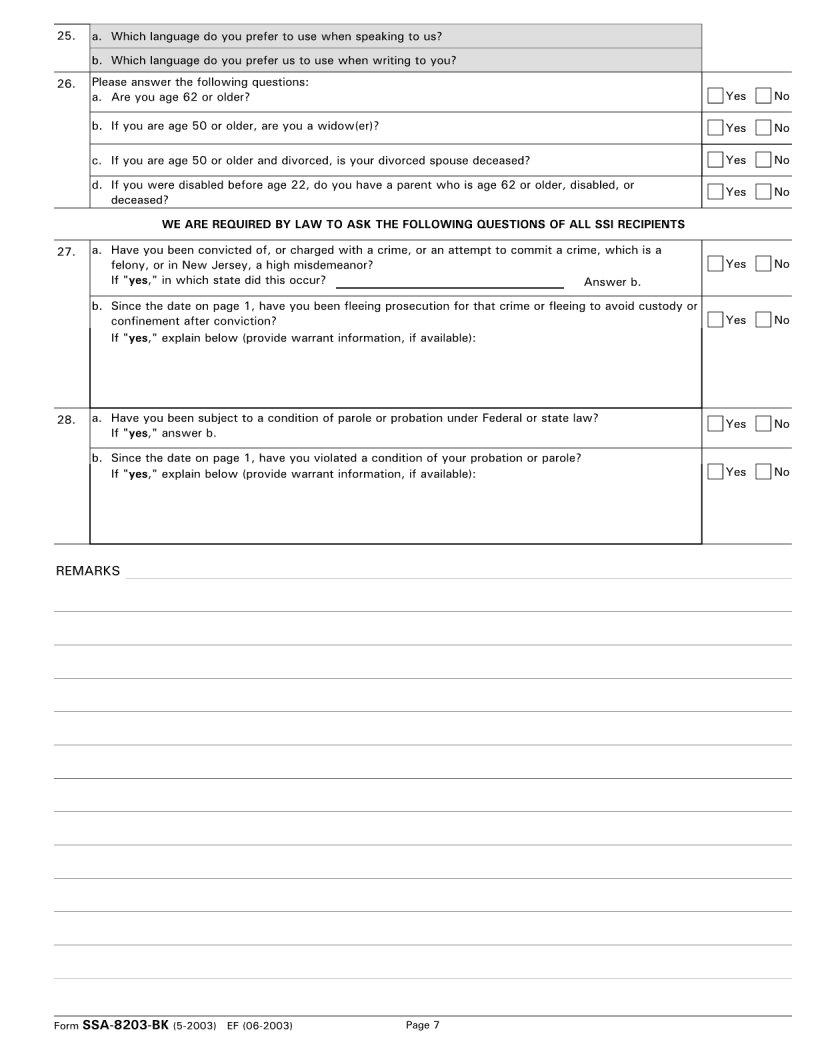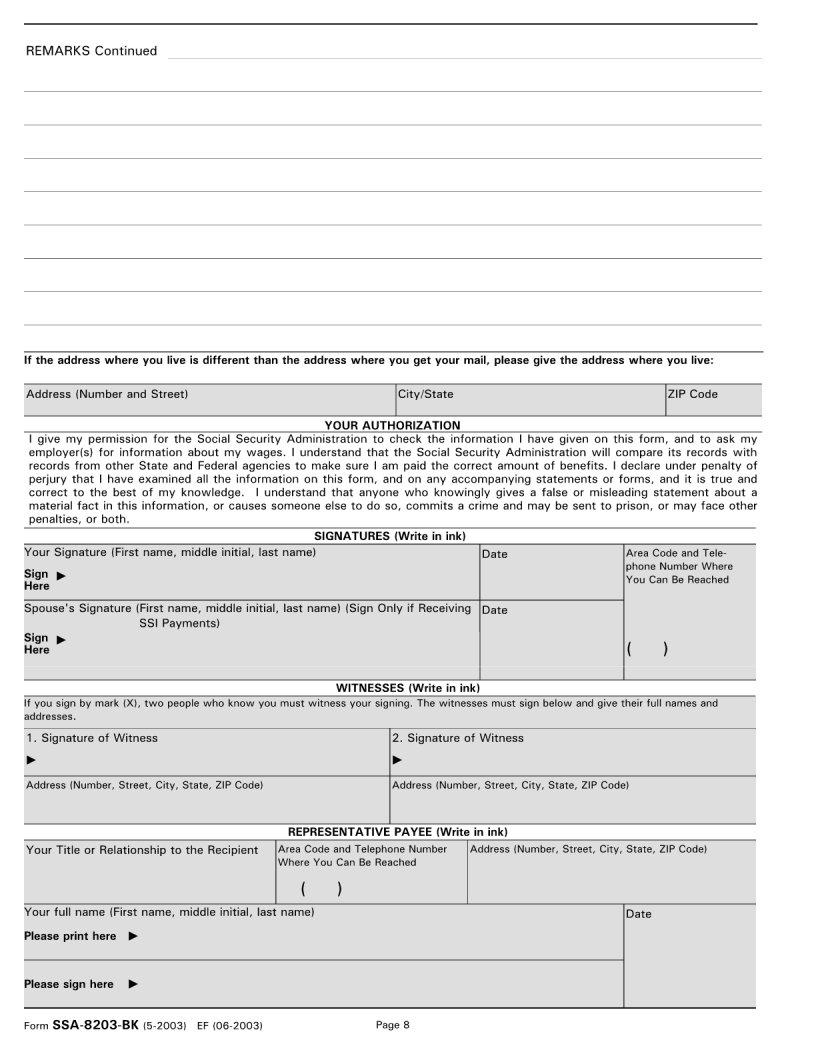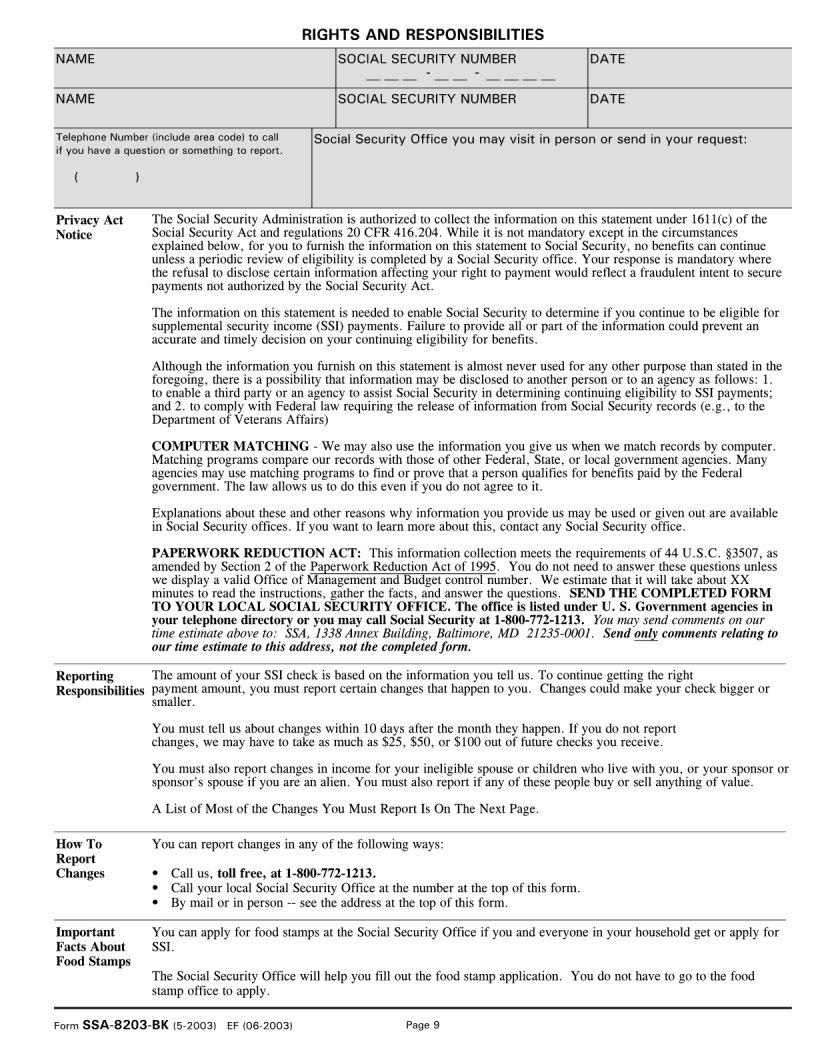
Understanding the intricacies of Social Security benefits is pivotal for individuals navigating their retirement or dealing with disabilities. Within this realm, the SSA 8203 BK form plays a crucial role. It is specifically designed for those receiving Supplemental Security Income (SSI) and is a tool used by the Social Security Administration (SSA) to assess an individual’s eligibility and ensure the accurate delivery of benefits. This form gathers detailed information about income, resources, living arrangements, and other personal details that can affect one's SSI benefits. The careful completion of this form can sometimes feel daunting due to its comprehensive nature, but it serves an essential purpose in maintaining the integrity of the SSI program and helping recipients receive the correct benefit amount. Whether an individual is applying for the first time or undergoing a routine review, the SSA 8203 BK form is a key component in the administration of their benefits, illuminating the financial and personal circumstances that directly influence eligibility and payment levels.
| Question | Answer |
|---|---|
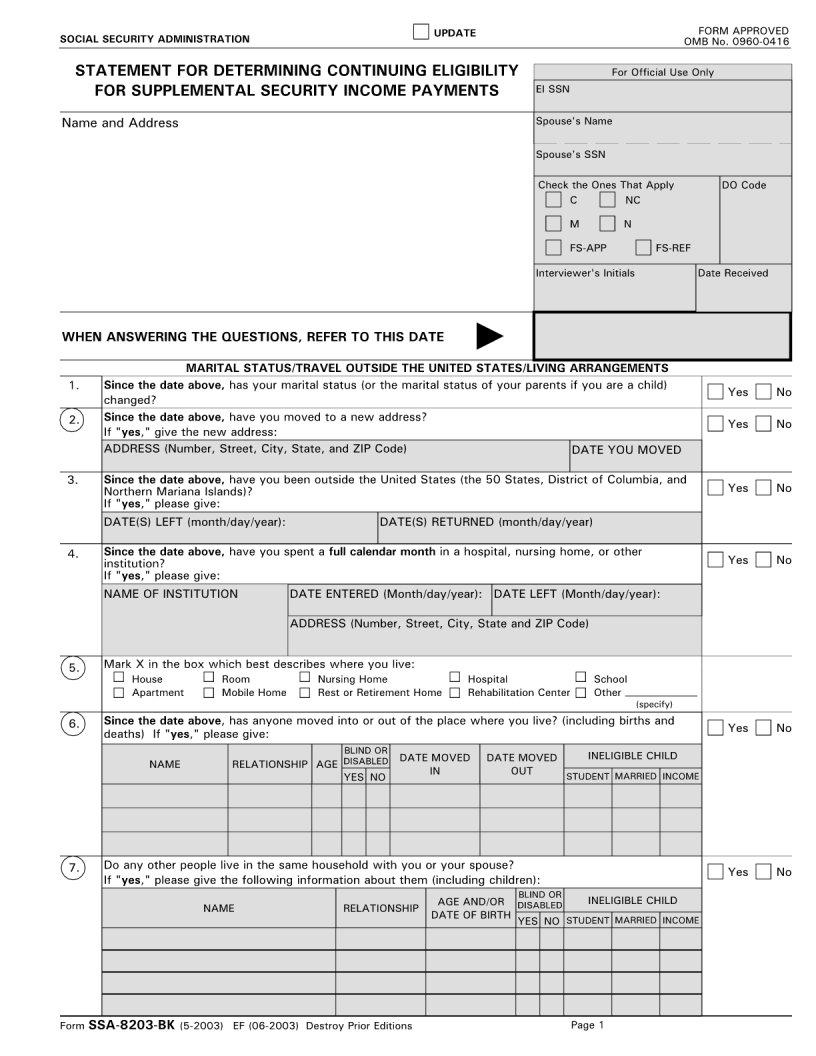
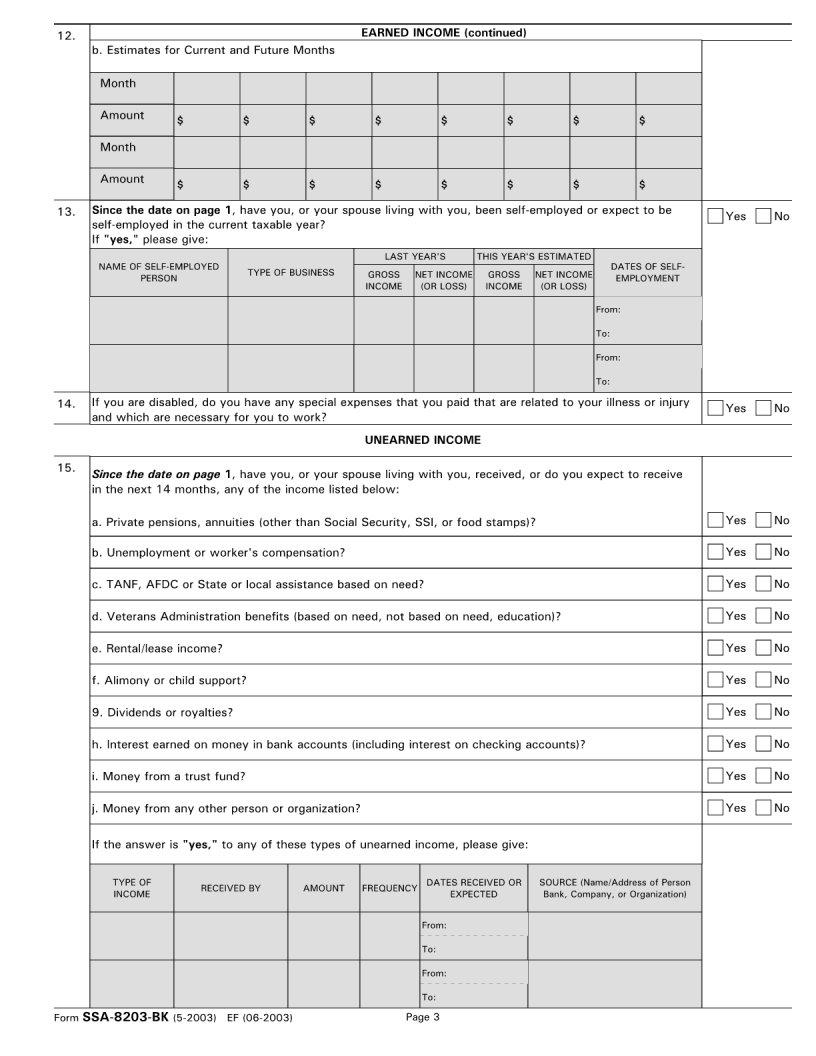
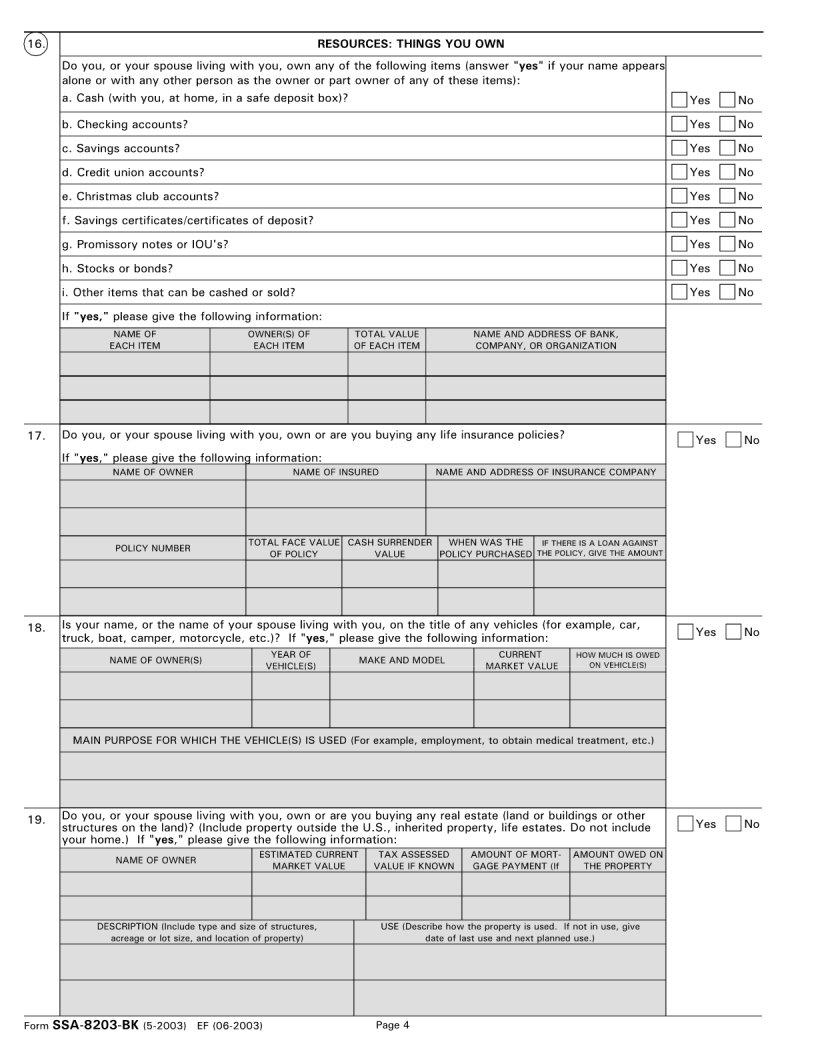
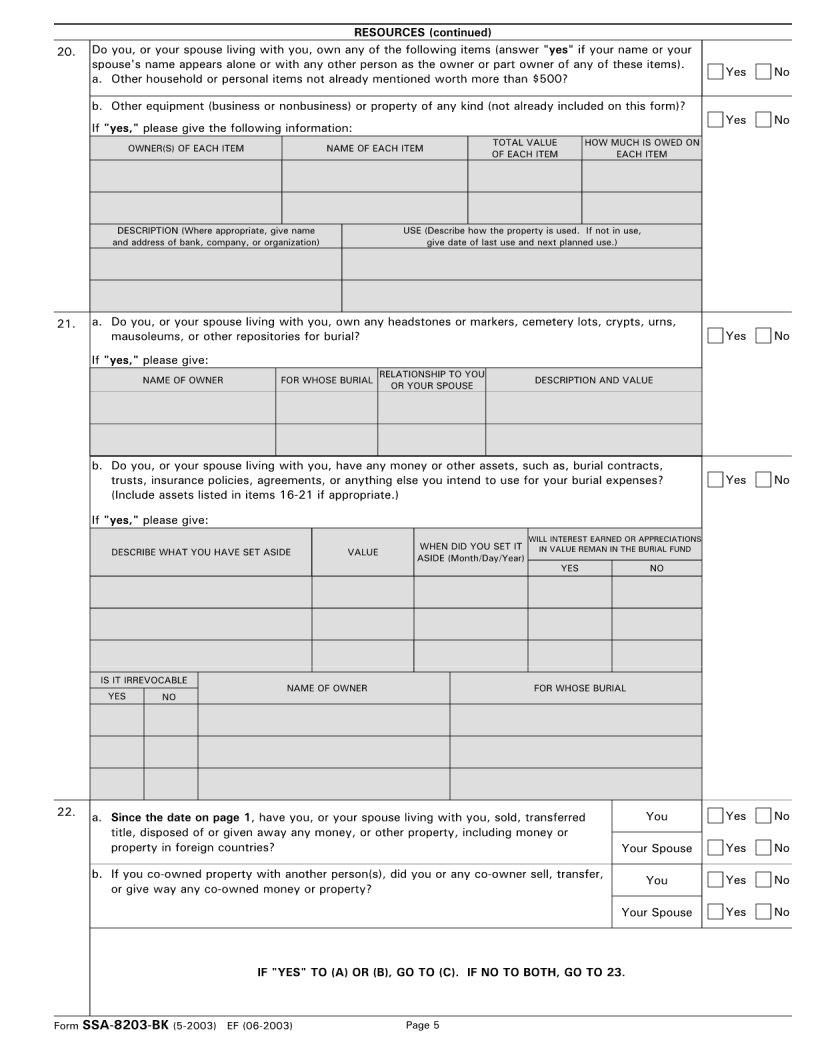
| Form Name | Form SSA-8203-BK |
| Form Length | 10 pages |
| Fillable? | Yes |
| Fillable fields | 591 |
| Avg. time to fill out | 30 min 11 sec |
| Other names | 8203 form, form 8203, socis security form 8203, ssa 8203 bk |