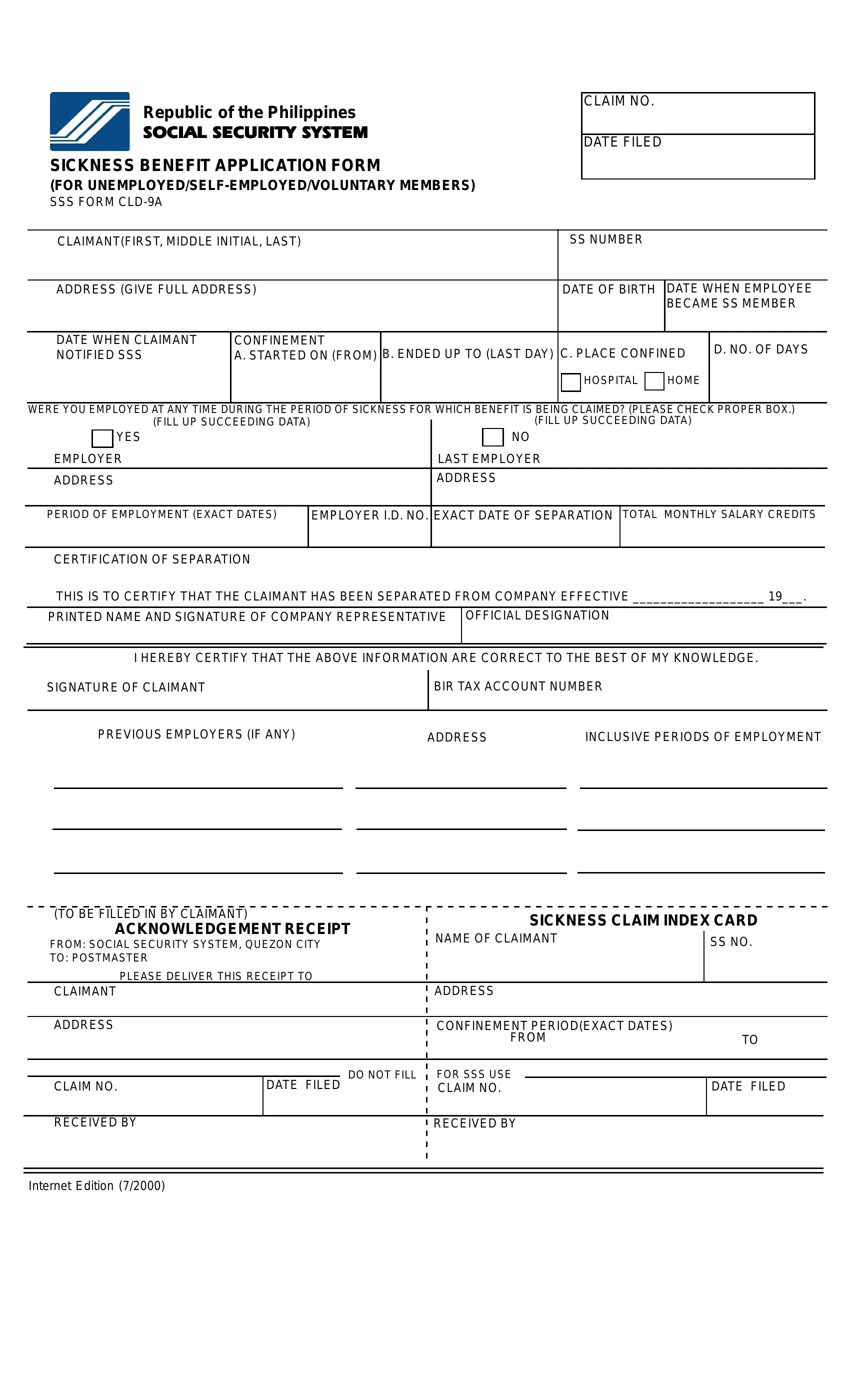
In navigating the complexities of social welfare and insurance benefits, certain documents play pivotal roles, acting as gatekeepers to entitled support and aid. Among these, the Social Security System Sickness Benefit Application Form, designated as SSS Form CLD-9A, stands out for those it specifically serves: unemployed, self-employed, and voluntary members in the Philippines. This form is a cornerstone for individuals seeking to claim sickness benefits, detailing the necessary information ranging from personal details to the specifics of their sickness period and employment history, if applicable. It meticulously outlines the requirement for a signature of claimant, evidence of the claim period through dates of confinement, details of any employment during the sickness period, and, importantly, the certification of separation for those who were employed. Further, the form includes instructions that emphasize the submission process, the conditions for necessary documentation given various employment scenarios, and a careful note on how to calculate relevant salary credits for the claim. Such precision in the form's design underscores its role not only as a procedural necessity but as a bridge for eligible claimants to access their duly benefits amidst trying times of illness, underscoring the social safety nets in place within the country's social security system.
| Question | Answer |
|---|---|
| Form Name | Sss Form Cld 9A |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | sickness notification, sickness reimbursement form, sss bank enrollment form, sss sickness maternity benefits payment thru the bank form 2019 |
Republic of the Philippines
SOCIAL SECURITY SYSTEM
SICKNESS BENEFIT APPLICATION FORM
(FOR
SSS FORM
CLAIM NO.
DATE FILED
CLAIMANT(FIRST, MIDDLE INITIAL, LAST) |
SS NUMBER |
|
|||
|
|
|
|||
ADDRESS (GIVE FULL ADDRESS) |
DATE OF BIRTH |
DATE WHEN EMPLOYEE |
|||
|
|
|
BECAME SS MEMBER |
||
|
|
|
|
|
|
DATE WHEN CLAIMANT |
CONFINEMENT |
|
|
D. NO. OF DAYS |
|
NOTIFIED SSS |
A. STARTED ON (FROM) B. ENDED UP TO (LAST DAY) C. PLACE CONFINED |
||||
|
|||||
HOSPITAL
HOME
WERE YOU EMPLOYED AT ANY TIME DURING THE PERIOD OF SICKNESS FOR WHICH BENEFIT IS BEING CLAIMED? (PLEASE CHECK PROPER BOX.)
|
|
(FILL UP SUCCEEDING DATA) |
|
|
(FILL UP SUCCEEDING DATA) |
|
|
YES |
|
|
NO |
EMPLOYER |
LAST EMPLOYER |
||||
|
|
|
|
|
|
ADDRESS |
ADDRESS |
||||
PERIOD OF EMPLOYMENT (EXACT DATES)
EMPLOYER I.D. NO. EXACT DATE OF SEPARATION
TOTAL MONTHLY SALARY CREDITS
CERTIFICATION OF SEPARATION
THIS IS TO CERTIFY THAT THE CLAIMANT HAS BEEN SEPARATED FROM COMPANY EFFECTIVE ___________________ 19___.
PRINTED NAME AND SIGNATURE OF COMPANY REPRESENTATIVE OFFICIAL DESIGNATION
I HEREBY CERTIFY THAT THE ABOVE INFORMATION ARE CORRECT TO THE BEST OF MY KNOWLEDGE. BIR TAX ACCOUNT NUMBER
|
|
|
|
|
|
|
|
|
PREVIOUS EMPLOYERS (IF ANY) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
INCLUSIVE PERIODS OF EMPLOYMENT |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(TO BE FILLED IN BY CLAIMANT)
ACKNOWLEDGEMENT RECEIPT
FROM: SOCIAL SECURITY SYSTEM, QUEZON CITY
TO: POSTMASTER
PLEASE DELIVER THIS RECEIPT TO
SICKNESS CLAIM INDEX CARD
NAME OF CLAIMANT |
SS NO. |
|
|
CLAIMANT
ADDRESS
ADDRESS
CONFINEMENT PERIOD(EXACT DATES) |
|
FROM |
TO |
CLAIM NO.
DO NOT FILL
DATE FILED
FOR SSS USE
CLAIM NO.
DATE FILED
RECEIVED BY
RECEIVED BY
Internet Edition (7/2000)
INSTRUCTIONS
1.Submit only one (1) copy. Avoid erasures or alterations.
2.If personally filed, submit this SSS form directly to the SSS Medical Evaluation Department.
3.If confined member is a married woman, print reported name at coverage.
4.Fill in the dates required in the format
5.Certification of separation is not necessary when the company is on strike, dissolved or closed, or when there is a case pending before a court regarding separation of the claimant. The following table shows the document required for any of these cases:
|
CONDITION |
DOCUMENT REQUIRED |
a. |
Company on strike |
Certification from CIR or Department of Labor and |
|
|
Employment |
b. |
Company dissolved or closed |
Affidavit by the claimant to this effect |
c. |
Pending case before a court |
Certification from the court |
6.The
CONFINEMENT |
PERIOD |
January to March 1998 April to June 1998 July to September 1998 October to December 1998
October 1996 to September 1997 January 1997 to December 1997 April 1997 to March 1998
July 1997 to June 1998