|
|
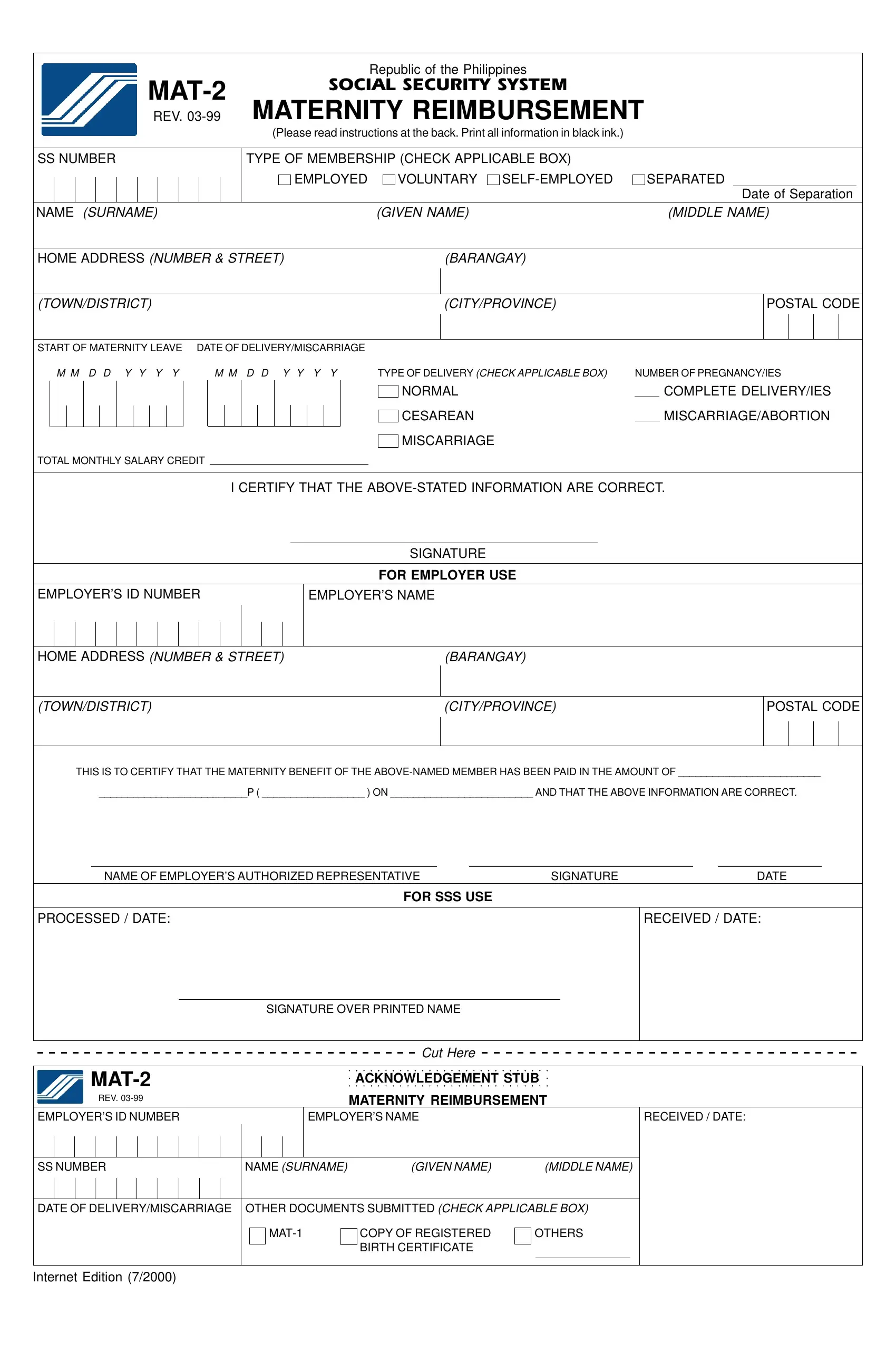
Republic of the Philippines |
|
MAT-2 |
SOCIAL SECURITY SYSTEM |
|
MATERNITY REIMBURSEMENT |
|
REV. 03-99 |
|
|
(Please read instructions at the back. Print all information in black ink.) |
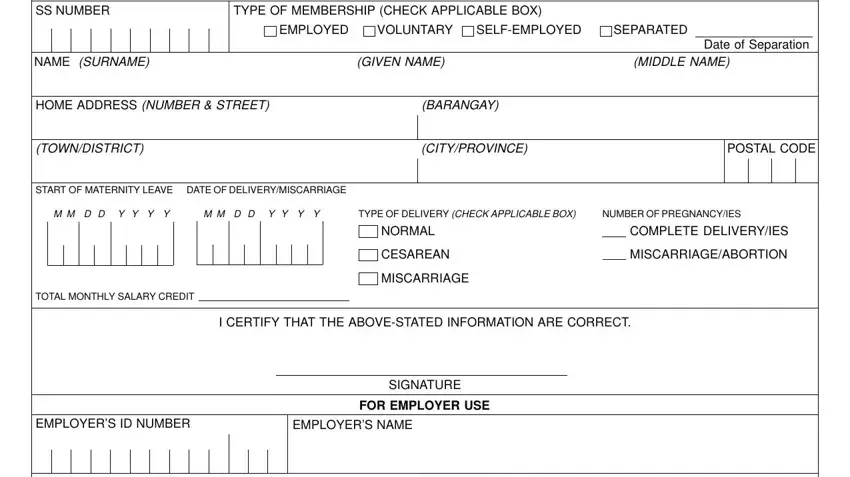
TYPE OF MEMBERSHIP (CHECK APPLICABLE BOX)
EMPLOYED |
VOLUNTARY SELF-EMPLOYED |
SEPARATED |
Date of Separation
NAME (SURNAME) |
(GIVEN NAME) |
(MIDDLE NAME) |
|
|
|
HOME ADDRESS (NUMBER & STREET) |
(BARANGAY) |
|
(TOWN/DISTRICT) |
(CITY/PROVINCE) |
START OF MATERNITY LEAVE |
DATE OF DELIVERY/MISCARRIAGE |
|
|
|
|
M M D D Y Y Y Y |
|
M M D D Y Y Y Y |
TYPE OF DELIVERY (CHECK APPLICABLE BOX) |
NUMBER OF PREGNANCY/IES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NORMAL |
|
COMPLETE DELIVERY/IES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CESAREAN |
|
MISCARRIAGE/ABORTION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MISCARRIAGE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TOTAL MONTHLY SALARY CREDIT |
|
|
|
|
I CERTIFY THAT THE ABOVE-STATED INFORMATION ARE CORRECT.
SIGNATURE
FOR EMPLOYER USE
HOME ADDRESS (NUMBER & STREET) |
(BARANGAY) |
(TOWN/DISTRICT) |
(CITY/PROVINCE) |
THIS IS TO CERTIFY THAT THE MATERNITY BENEFIT OF THE ABOVE-NAMED MEMBER HAS BEEN PAID IN THE AMOUNT OF _________________________
__________________________P ( __________________ ) ON _________________________ AND THAT THE ABOVE INFORMATION ARE CORRECT.
NAME OF EMPLOYER’S AUTHORIZED REPRESENTATIVE |
SIGNATURE |
DATE |
FOR SSS USE
SIGNATURE OVER PRINTED NAME
Cut Here
|
|
MAT-2 |
|
|
|
|
ACKNOWLEDGEMENT STUB |
|
|
|
REV. 03-99 |
|
|
|
|
MATERNITY REIMBURSEMENT |
EMPLOYER’S ID NUMBER |
|
|
|
EMPLOYER’S NAME |
|
|
RECEIVED / DATE: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SS NUMBER |
NAME (SURNAME) |
(GIVEN NAME) |
(MIDDLE NAME) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF DELIVERY/MISCARRIAGE |
OTHER DOCUMENTS SUBMITTED (CHECK APPLICABLE BOX) |
|
|
|
|
|
|
|
|
|
|
|
|
MAT-1 |
COPY OF REGISTERED |
OTHERS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BIRTH CERTIFICATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Internet Edition (7/2000)
INSTRUCTIONS AND REMINDERS
1.Accomplish and submit this form in one copy.
2.Any alteration should be initialed by the member or the employer’s authorized representative, if employed.
3.Maternity benefits can be availed only by FEMALE SSS members.
4.Maternity benefits must be advanced by the employer to the employee within 30 days from the filing of the maternity leave application.
5.Payment of maternity benefits disqualifies you automatically from availing of sickness benefits for the same period for which maternity benefits have been received.
6.Effective May 24, 1997, maternity benefits shall be paid only for the first four deliveries or miscarriages. The fifth complete delivery or miscarriage shall no longer be paid even if no availments were made on previous deliveries.
REQUIREMENTS
1.Maternity notification duly stamped received by the SSS prior to the date of childbirth/miscarriage
2.The member must have paid at least three monthly contributions within the 12 month period immediately preceding the semester of childbirth or miscarriage.
3.a. For Normal Delivery
•Certified true copy or authenticated copy of Birth Certificate duly registered with the Local Civil Registrar.
b.For Cesarean Delivery
•Certified true copy or authenticated copy of Birth Certificate duly registered with the Local Civil Registrar.
•Operating Room Record or Surgical Memorandum duly certified by the hospital where the member is confined.
c.For Stillbirth
•Fetal Death Certificate duly registered with the Local Civil Registrar.
d.For Miscarriage or Abortion
•Pregnancy test before and after miscarriage/abortion.
•Medical Certificate/Obstetrical history indicating the number of miscarriages duly certified by the attending physician with his license number, printed name and signature; or
•D & C Report duly certified by the authorized hospital representative where the member was confined.
4.a. For Separated Member
•Certification from last employer with the effective date of separation from employment. b. For Voluntary Member
•a copy of approved SS Form E-5
c. For Self-employed Member
•a copy of approved SS Form RS-1
COMPUTATION OF MATERNITY BENEFIT
1.Exclude the semester of contingency (Delivery, Miscarriage or Abortion) (Semester refers to two successive quarters ending in the quarter of contingency)
2.Count 12 months backward starting from the month immediately preceding the semester of contingency.
3.Identify and add the six highest Monthly Salary Credits (MSC) within the 12 month period preceding the semester of contingency.
4.Divide the total MSCs by 180 days to arrive at the Daily Maternity Allowance.
5.Multiply the Daily Maternity Allowance by 60 for normal delivery or miscarriage or 78 days for cesarean delivery to get the total maternity benefit.
However, in case a member dies before the lapse of 60 or 78 days from the date of contingency, the number of days to be considered in the computation should be from the start of the employee’s maternity leave up to the day prior to the date of death.
Example: |
Contingency - August 5, 1998 |
|
Start of Maternity Leave - August 1, 1998 |
1.The semester of contingency is April 1998 to Sept. 1998.
2.The 12 month period prior to the semester of contingency is April 1997 to March 1998.
3.The total MSC which is the total of the of the six highest MSC’s is 63,000 (10,000 x 3) + (11,000 x 3).
4.The Daily Maternity Allowance would be 350.00 (63,000 / 180).
5.The maternity benefit due to the member would be P21,000 (350.00 x 60) in case of normal delivery/miscarriage and P27,300 (350.00 x 78) in case of cesarean delivery.
In case the member died on August 31, 1998, the maternity benefit due is P10,500 (350.00 x 30) i.e. August 1, 1998 to August 30, 1998.