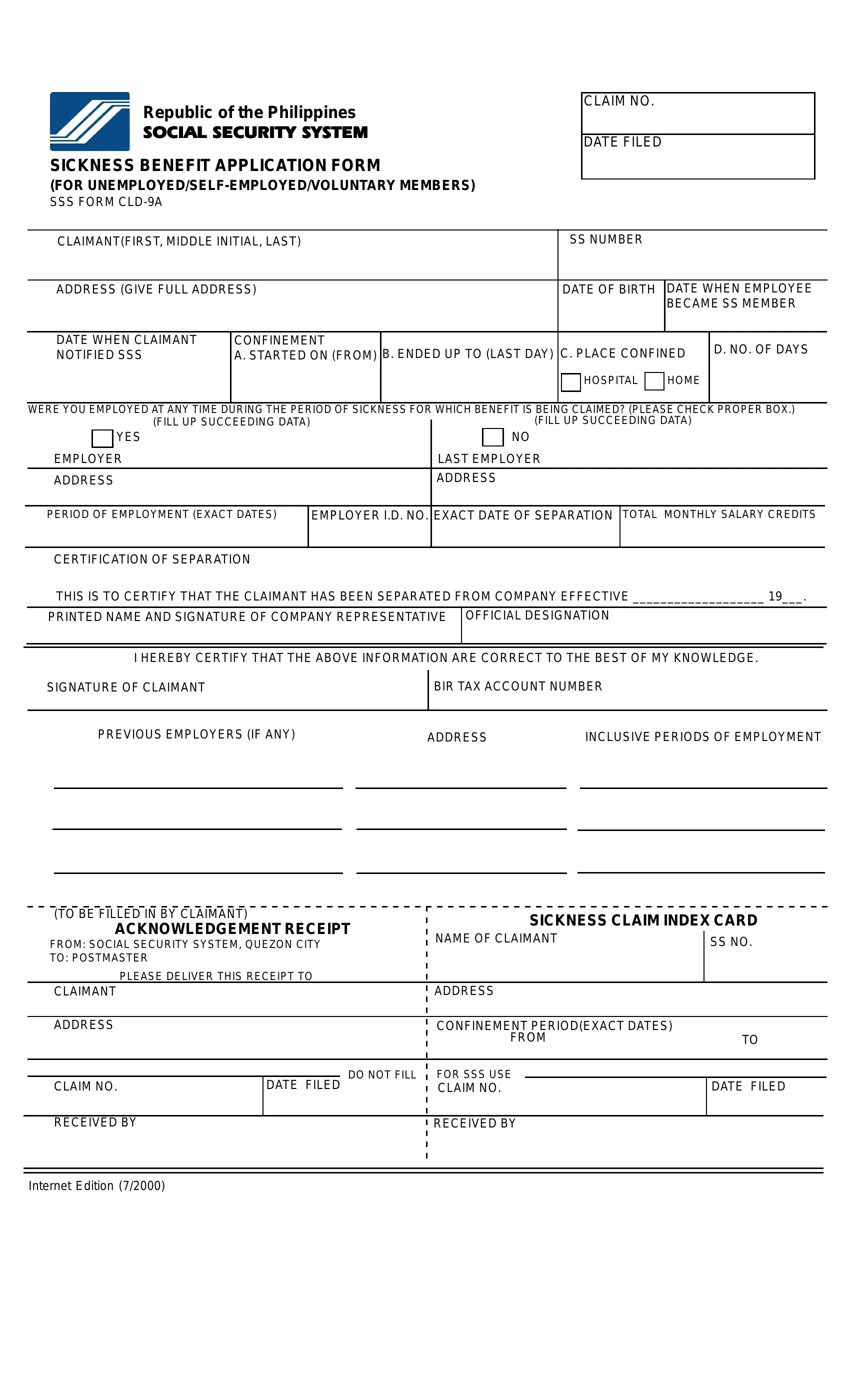
In navigating the complexities of social welfare and insurance benefits, certain documents play pivotal roles, acting as gatekeepers to entitled support and aid. Among these, the Social Security System Sickness Benefit Application Form, designated as SSS Form CLD-9A, stands out for those it specifically serves: unemployed, self-employed, and voluntary members in the Philippines. This form is a cornerstone for individuals seeking to claim sickness benefits, detailing the necessary information ranging from personal details to the specifics of their sickness period and employment history, if applicable. It meticulously outlines the requirement for a signature of claimant, evidence of the claim period through dates of confinement, details of any employment during the sickness period, and, importantly, the certification of separation for those who were employed. Further, the form includes instructions that emphasize the submission process, the conditions for necessary documentation given various employment scenarios, and a careful note on how to calculate relevant salary credits for the claim. Such precision in the form's design underscores its role not only as a procedural necessity but as a bridge for eligible claimants to access their duly benefits amidst trying times of illness, underscoring the social safety nets in place within the country's social security system.
| Question | Answer |
|---|---|
| Form Name | Sss Form Cld 9A |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | sickness notification, sickness reimbursement form, sss bank enrollment form, sss sickness maternity benefits payment thru the bank form 2019 |
