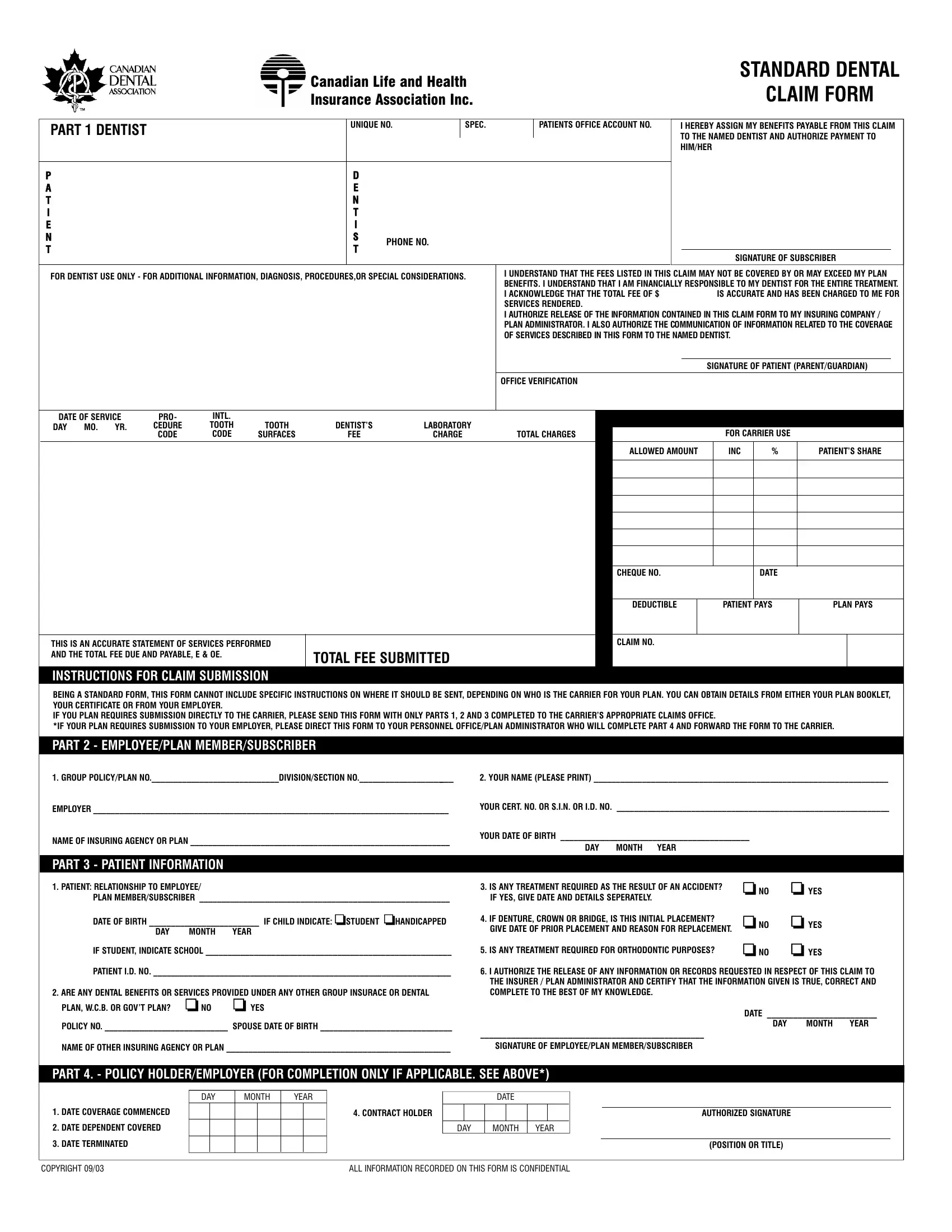
Dealing with dental treatments can lead to a maze of paperwork and procedures, but understanding the Standard Dental Canadian Life and Health Insurance Association Inc. Claim Form can help navigate this process. Typically, when patients receive dental care, this form becomes a bridge between the dental office, the patient, and the insurance company. It acts as a comprehensive document where dentists can assign benefits payable from the claim directly to themselves, ensuring they receive payment for services rendered. Importantly, patients acknowledge their financial responsibility for the treatment, a crucial step in the process. This form also includes specific sections for the dentist's use, such as additional information, diagnosis, procedures, or special considerations related to the patient's treatment. The submission instructions vary, depending on the insurance carrier and whether the submission is direct or through an employer, underlining the need for clear communication and accurate completion of the form. The form covers details from patient information, insurance details, treatment required, and authorization for the release of information, aiming to streamline the claim process for everyone involved. Whether you're a patient, a dental office professional, or someone managing employee benefits, understanding the parts and purpose of this form can significantly ease the process of submitting dental claims.
| Question | Answer |
|---|---|
| Form Name | Standard Dental Claim Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | standard ada form, standard dental claim form, SEPERATELY, claim |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STANDARD DENTAL |
|||||
|
|
|
|
|
|
|
|
|
|
|
CANADIAN LIFE AND HEALTH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CLAIM FORM |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
INSURANCE ASSOCIATION INC. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
UNIQUE NO. |
|
SPEC. |
|
|
|
PATIENTS OFFICE ACCOUNT NO. |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
PART 1 DENTIST |
|
|
|
|
|
|
|
|
|
|
|
I HEREBY ASSIGN MY BENEFITS PAYABLE FROM THIS CLAIM |
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TO THE NAMED DENTIST AND AUTHORIZE PAYMENT TO |
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HIM/HER |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
P |
|
|
|
|
|
|
|
|
|
|
D |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
A |
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
T |
|
|
|
|
|
|
|
|
|
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I |
|
|
|
|
|
|
|
|
|
|
T |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N |
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PHONE NO. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
T |
|
|
|
|
|
|
|
|
|
|
T |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SIGNATURE OF SUBSCRIBER |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FOR DENTIST USE ONLY - FOR ADDITIONAL INFORMATION, DIAGNOSIS, PROCEDURES,OR SPECIAL CONSIDERATIONS. |
|
|
|
I UNDERSTAND THAT THE FEES LISTED IN THIS CLAIM MAY NOT BE COVERED BY OR MAY EXCEED MY PLAN |
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
BENEFITS. I UNDERSTAND THAT I AM FINANCIALLY RESPONSIBLE TO MY DENTIST FOR THE ENTIRE TREATMENT. |
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I ACKNOWLEDGE THAT THE TOTAL FEE OF $ |
|
|
|
|
IS ACCURATE AND HAS BEEN CHARGED TO ME FOR |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SERVICES RENDERED. |
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I AUTHORIZE RELEASE OF THE INFORMATION CONTAINED IN THIS CLAIM FORM TO MY INSURING COMPANY / |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLAN ADMINISTRAT O R. I ALSO AUTHORIZE THE COMMUNICATION OF INFORMATION RELATED TO THE COVERAGE |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OF SERVICES DESCRIBED IN THIS FORM TO THE NAMED DENTIST. |
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SIGNATURE OF PATIENT (PARENT/GUARDIAN) |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OFFICE VERIFICATION |
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF SERVICE |
|
PRO- |
INTL. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
DAY |
MO. |
YR. |
|
CEDURE |
TOOTH |
TOOTH |
|
DENTIST’S |
|
LABORATORY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FOR CARRIER USE |
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
CODE |
CODE |
SURFACES |
|
|
FEE |
|
CHARGE |
|
|
TOTAL CHARGES |
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ALLOWED AMOUNT |
|
INC |
% |
PATIENT’S SHARE |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CHEQUE NO.
DATE
THIS IS AN ACCURATE STATEMENT OF SERVICES PERFORMED AND THE TOTAL FEE DUE AND PAYABLE, E & OE.
INSTRUCTIONS FOR CLAIM SUBMISSION
DEDUCTIBLE |
PATIENT PAYS |
PLAN PAYS |
|
|
|
CLAIM NO.
TOTAL FEE SUBMITTED
BEING A STANDARD FORM, THIS FORM CANNOT INCLUDE SPECIFIC INSTRUCTIONS ON WHERE IT SHOULD BE SENT, DEPENDING ON WHO IS THE CARRIER FOR YOUR PLAN. YOU CAN OBTAIN DETAILS FROM EITHER YOUR PLAN BOOKLET, YOUR CERTIFICATE OR FROM YOUR EMPLOYER.
IF YOU PLAN REQUIRES SUBMISSION DIRECTLY TO THE CARRIER, PLEASE SEND THIS FORM WITH ONLY PARTS 1, 2 AND 3 COMPLETED TO THE CARRIER’S APPROPRIATE CLAIMS OFFICE.
*IF YOUR PLAN REQUIRES SUBMISSION TO YOUR EMPLOYER, PLEASE DIRECT THIS FORM TO YOUR PERSONNEL OFFICE/PLAN ADMINISTRATOR WHO WILL COMPLETE PART 4 AND FORWARD THE FORM TO THE CARRIER.
PART 2 - EMPLOYEE/PLAN MEMBER/SUBSCRIBER
1.GROUP POLICY/PLAN NO._____________________________DIVISION/SECTION NO.______________________
EMPLOYER _________________________________________________________________________________
NAME OF INSURING AGENCY OR PLAN ___________________________________________________________
PART 3 - PATIENT INFORMATION
1. PATIENT: RELATIONSHIP TO EMPLOYEE/
PLAN MEMBER/SUBSCRIBER _________________________________________________________
DATE OF BIRTH _________________________ IF CHILD INDICATE: ❏STUDENT ❏HANDICAPPED
DAY |
MONTH |
YEAR |
IF STUDENT, INDICATE SCHOOL ________________________________________________________ |
||
PATIENT I.D. NO. ____________________________________________________________________ |
||
2. ARE ANY DENTAL BENEFITS OR SERVICES PROVIDED UNDER ANY OTHER GROUP INSURACE OR DENTAL |
||
PLAN, W.C.B. OR GOV’T PLAN? |
❏ NO |
❏ YES |
POLICY NO. ____________________________ SPOUSE DATE OF BIRTH ______________________________
NAME OF OTHER INSURING AGENCY OR PLAN ___________________________________________________
2.YOUR NAME (PLEASE PRINT) ___________________________________________________________________
YOUR CERT. NO. OR S.I.N. OR I.D. NO. ______________________________________________________________
YOUR DATE OF BIRTH ___________________________________________ |
|
|||
|
DAY |
MONTH YEAR |
|
|
3. |
IS ANY TREATMENT REQUIRED AS THE RESULT OF AN ACCIDENT? |
❏ NO |
❏ YES |
|
|
IF YES, GIVE DATE AND DETAILS SEPERATELY. |
|
|
|
4. |
IF DENTURE, CROWN OR BRIDGE, IS THIS INITIAL PLACEMENT? |
❏ NO |
❏ YES |
|
|
GIVE DATE OF PRIOR PLACEMENT AND REASON FOR REPLACEMENT. |
|||
|
|
|
||
5. |
IS ANY TREATMENT REQUIRED FOR ORTHODONTIC PURPOSES? |
❏ NO |
❏ YES |
|
6.I AUTHORIZE THE RELEASE OF ANY INFORMATION OR RECORDS REQUESTED IN RESPECT OF THIS CLAIM TO THE INSURER / PLAN ADMINISTRATOR AND CERTIFY THAT THE INFORMATION GIVEN IS TRUE, CORRECT AND COMPLETE TO THE BEST OF MY KNOWLEDGE.
DATE _________________________
DAY MONTH YEAR
___________________________________________________
SIGNATURE OF EMPLOYEE/PLAN MEMBER/SUBSCRIBER
PART 4. - POLICY HOLDER/EMPLOYER (FOR COMPLETION ONLY IF APPLICABLE. SEE ABOVE*)
DAY
1.DATE COVERAGE COMMENCED
2.DATE DEPENDENT COVERED
3.DATE TERMINATED
MONTH
YEAR |
DATE |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
4. CONTRACT HOLDER |
|
|
|
|
|
|
|
AUTHORIZED SIGNATURE |
|
|
DAY |
MONTH |
YEAR |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(POSITION OR TITLE) |
COPYRIGHT 09/03 |
ALL INFORMATION RECORDED ON THIS FORM IS CONFIDENTIAL |