
Handling PDF files online is certainly a breeze using our PDF tool. You can fill in LSD here and try out various other functions available. To make our editor better and more convenient to utilize, we continuously come up with new features, taking into consideration feedback coming from our users. It just takes a few simple steps:
Step 1: Just click on the "Get Form Button" at the top of this site to see our pdf form editing tool. There you will find all that is necessary to fill out your document.
Step 2: Once you access the online editor, you will see the document made ready to be completed. Besides filling out various blank fields, you could also do other sorts of actions with the file, such as putting on your own text, modifying the initial text, inserting images, signing the PDF, and much more.
This document will need some specific information; to ensure correctness, don't hesitate to bear in mind the subsequent tips:
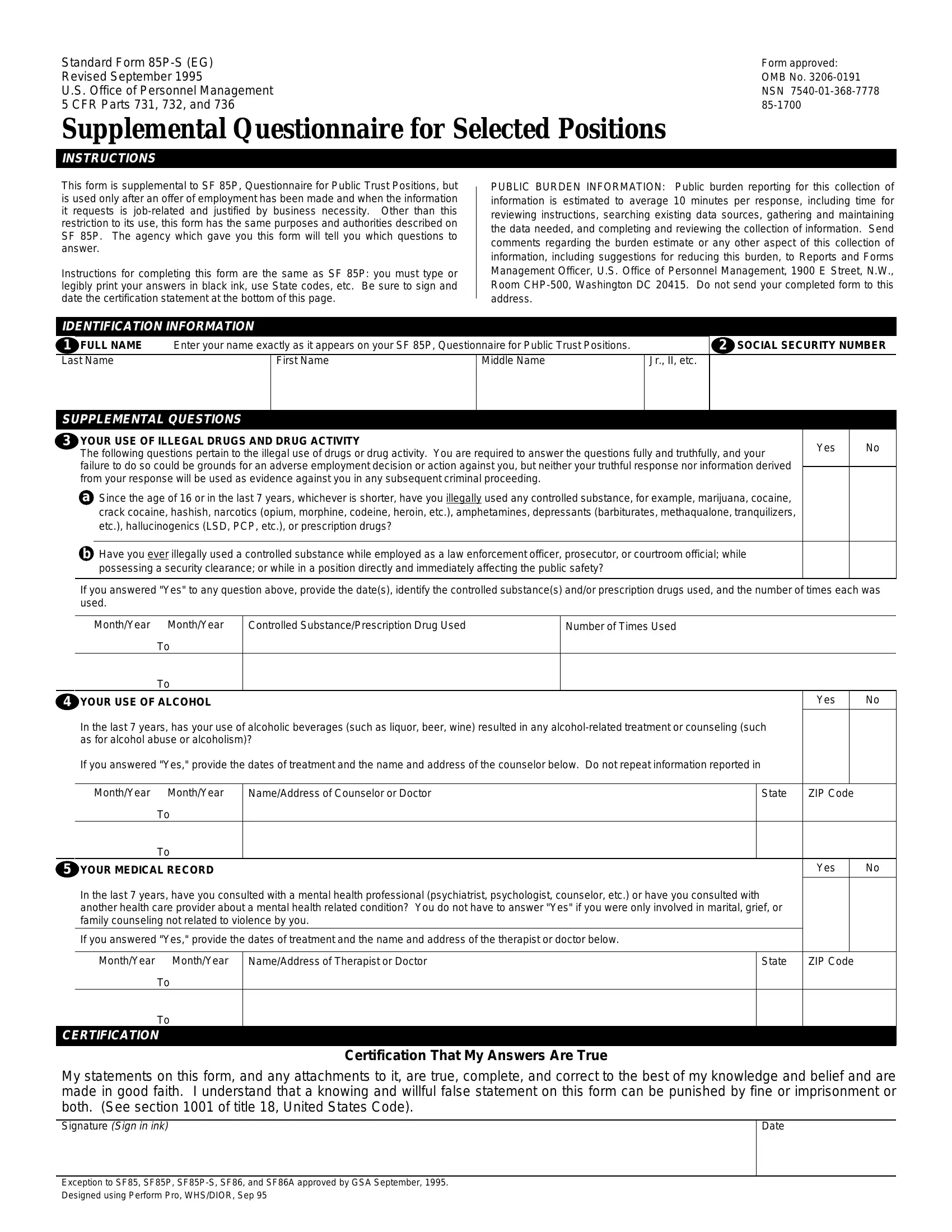
1. Start completing the LSD with a selection of essential blanks. Collect all of the important information and be sure nothing is overlooked!
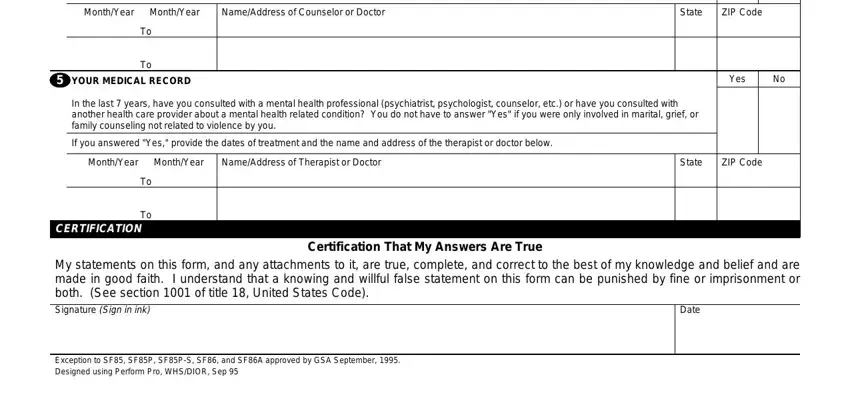
2. Once the first part is filled out, proceed to type in the suitable details in all these: MonthYear, MonthYear, NameAddress of Counselor or Doctor, State, ZIP Code, YOUR MEDICAL RECORD, Yes, In the last years have you, If you answered Yes provide the, MonthYear, MonthYear, NameAddress of Therapist or Doctor, State, ZIP Code, and CERTIFICATION.
When it comes to MonthYear and Yes, make certain you do everything properly here. Both of these are definitely the most important fields in this PDF.
Step 3: Ensure that the details are correct and then press "Done" to finish the project. Make a 7-day free trial option at FormsPal and get instant access to LSD - download or edit inside your personal account page. FormsPal provides protected document editor devoid of data recording or distributing. Rest assured that your details are secure with us!