
RFD can be filled in online without difficulty. Simply try FormsPal PDF editing tool to perform the job in a timely fashion. We at FormsPal are aimed at making sure you have the absolute best experience with our tool by regularly presenting new functions and enhancements. Our tool has become a lot more user-friendly as the result of the newest updates! At this point, filling out documents is a lot easier and faster than ever. Getting underway is effortless! All that you should do is stick to the following easy steps below:
Step 1: Access the PDF in our tool by clicking on the "Get Form Button" in the top section of this webpage.
Step 2: The editor grants the capability to modify most PDF documents in many different ways. Transform it with your own text, correct what's originally in the file, and include a signature - all within the reach of a couple of clicks!
This PDF will need specific information to be filled out, thus you need to take your time to provide exactly what is requested:
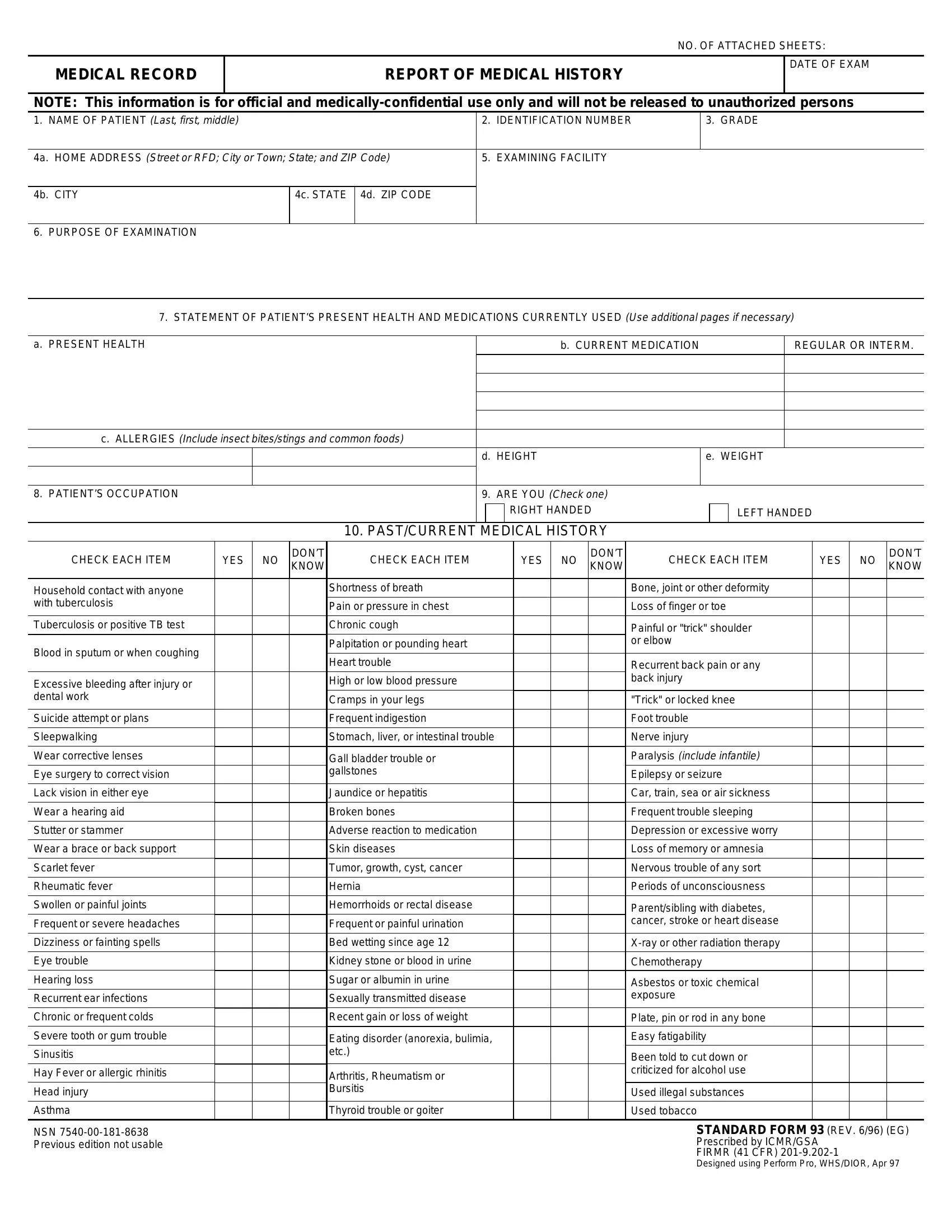
1. To begin with, while filling out the RFD, beging with the part containing next blanks:
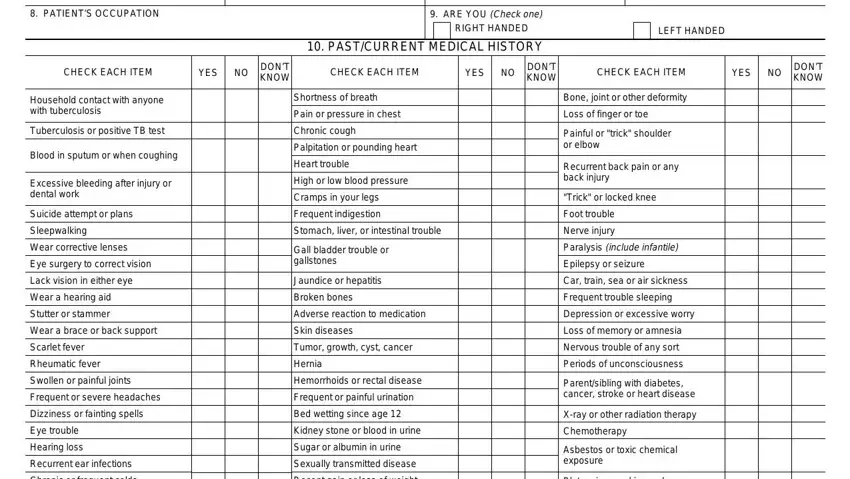
2. Right after performing the last section, go to the subsequent stage and fill in all required details in all these blank fields - PATIENTS OCCUPATION, ARE YOU Check one, RIGHT HANDED, PASTCURRENT MEDICAL HISTORY, LEFT HANDED, CHECK EACH ITEM, YES, DONT KNOW, CHECK EACH ITEM, YES, DONT KNOW, CHECK EACH ITEM, YES, DONT KNOW, and Household contact with anyone with.
3. Completing Suicide attempt or plans, NSN Previous edition not usable, Jaundice or hepatitis Broken bones, Eating disorder anorexia bulimia, Arthritis Rheumatism or Bursitis, Thyroid trouble or goiter, Plate pin or rod in any bone Easy, Been told to cut down or, Used illegal substances Used, and STANDARD FORM REV EG Prescribed is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. This specific section comes next with the next few blank fields to focus on: CHECK EACH ITEM, Treated for a female disorder, YES, DONT KNOW, DATE OF LAST MENSTRUAL PERIOD, DATE OF LAST PAP SMEAR DATE OF, GRAM, CHECK EACH ITEM IF YES EXPLAIN IN, YES, Have you been refused employment, a Sensitivity to chemicals dust, Have you ever been treated for a, Have you ever been denied life, Have you had or have you been, and Have you ever been a patient in.
5. This last stage to finish this document is crucial. Make sure to fill in the necessary blank fields, which includes Have you ever been discharged, Have you ever been arrested or, Have you ever been diagnosed with, LIST ALL IMMUNIZATIONS RECEIVED, I certify that I have reviewed the, b SIGNATURE, c DATE, NOTE HAND TO THE DOCTOR OR NURSE, a TYPED OR PRINTED NAME OF, b SIGNATURE, c DATE, and STANDARD FORM REV BACK, prior to using the file. Or else, it could end up in an incomplete and possibly invalid paper!
When it comes to c DATE and LIST ALL IMMUNIZATIONS RECEIVED, be certain that you review things in this current part. These two could be the key fields in this page.
Step 3: Spell-check the information you have typed into the blanks and press the "Done" button. Get hold of your RFD when you sign up for a 7-day free trial. Immediately get access to the pdf from your FormsPal account page, along with any modifications and adjustments being all saved! FormsPal provides protected form completion with no data recording or any kind of sharing. Be assured that your information is secure with us!