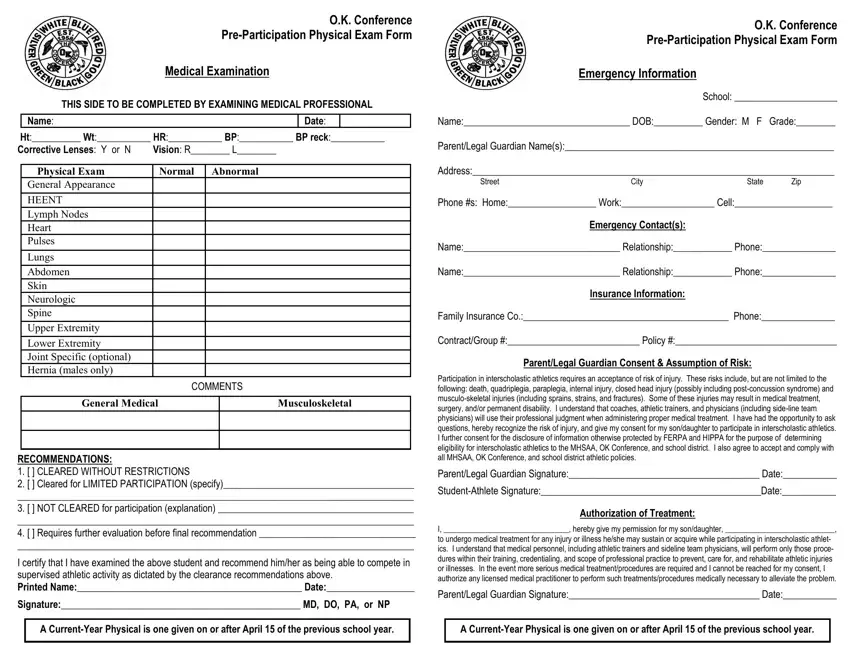
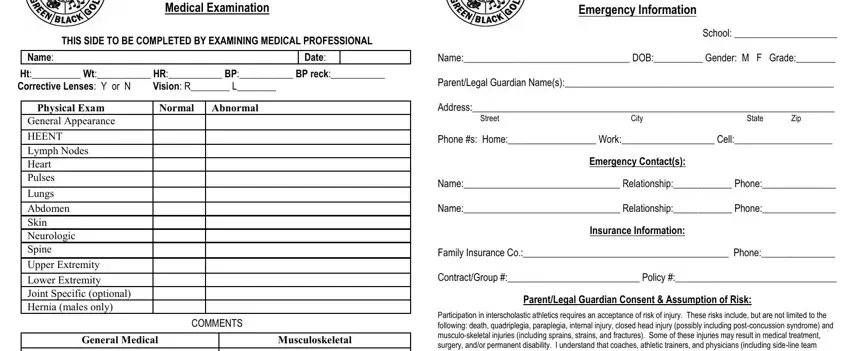
Medical History |
|
|
1. Do you have any chronic or ongoing medical conditions? |
Yes |
No |
If yes, explain:____________________________________________________________________
2. Have you ever been hospitalized and/or had surgery for any reason?Yes No If yes, explain:____________________________________________________________________
3. Do you have any allergies (medications, insects, foods, etc.)?Yes No If yes, explain:____________________________________________________________________
4. Are you currently taking any medications or supplements (include over-the-counter)? Yes No If yes, explain:____________________________________________________________________
5. Have you had a medical problem or injury since your last physical exam?Yes No If yes, explain;____________________________________________________________________
6. Have you ever passed out or nearly passed out during or after exercise? |
Yes |
No |
Have you ever had chest pain, tightness, or pressure during or after exercise? |
Yes |
No |
Have you ever been dizzy or light headed during or after exercise? |
Yes |
No |
Do you get more tired or short of breath than others during exercise? |
Yes |
No |
Does your heart ever race or skip beats (irregular beats) during exercise? |
Yes |
No |
Has a doctor ever ordered a test for your heart (e.g. ECG/EKG, echocardiogram? |
Yes |
No |
Have you ever been told you have any of the following (check all that apply):
High blood pressure |
Heart murmur |
High cholesterol |
A heart infection |
Kawasaki disease |
Other:_____________________ |
Explain ALL yes answers & checked items:_____________________________________________
_______________________________________________________________________________
7. Has anyone in your family died suddenly OR of heart problems before age 50? |
Yes |
No |
Do anyone in your family have a heart problem, pacemaker, or implanted defibrillator? Yes |
No |
Has anyone in your family had unexplained fainting, seizures, or near drowning? |
Yes |
No |
Does anyone in your family have any of the following cardiovascular conditions:
Hypertrophic cardiomyopathy |
Marfan syndrome |
Brugada syndrome |
Arrythmogenic right ventricular cardiomyopathy |
Long QT syndrome |
Catecholaminergic polymorphic ventricular tachycardia |
Short QT syndrome |
Explain ALL yes answers & checked items:_____________________________________________
_______________________________________________________________________________
8. Have you ever had a concussion, head injury, or recurrent headaches?Yes No If yes, explain:____________________________________________________________________
Have you ever been knocked out or unconscious?Yes No If yes, explain:____________________________________________________________________
Do you have headaches with exercise?Yes No If yes, explain:____________________________________________________________________
Have you ever had any of the following after a hit, blow to the head, or falling:
Confusion |
Prolonged headache |
Inability to move your arms or legs |
Memory problems Numbness, tingling, or weakness in your arms or legs
Explain ALL checked items (include dates):_____________________________________________
_______________________________________________________________________________
Have you ever had a stinger, burner, or pinched nerve?Yes No If yes, explain:____________________________________________________________________
Have you ever had seizures, convulsions, or a history of epilepsy?Yes No If yes, explain:____________________________________________________________________
9. Have you ever become ill, dizzy, or passed out while exercising in the heat?Yes No If yes, explain:____________________________________________________________________
Do you get frequent muscle or heat cramps when exercising?Yes No If yes, explain:____________________________________________________________________
Do you or someone in your family have sickle cell trait or disease?Yes No If yes, explain:____________________________________________________________________
10.Do you or someone in your family have asthma or another obstructive lung disorder? Yes No If yes, explain:____________________________________________________________________
Do you cough, wheeze, or have difficulty breathing during or after exercise?Yes No If yes, explain:____________________________________________________________________
Have you ever used an inhaler or taken asthma medication?Yes No If yes, explain:____________________________________________________________________
11.Do you currently have, or have you EVER HAD any of the following:
Hernia Mononucleosis Diabetes Kidney disease Scoliosis Absent spleen Explain ALL checked items (include dates):_____________________________________________
_______________________________________________________________________________
12.Are you missing one of a set of paired organs (kidneys, eyes, ovaries, testes, etc.)? Yes No If yes, explain:____________________________________________________________________
13.Have you ever sprained, strained, dislocated, fractured, broken, experienced repeated swelling in, had a stress fracture in, or otherwise injured any bones or joints? (check all that apply)
Head |
Neck |
Chest/ribs |
Back |
Shoulder |
Forearm |
Elbow Wrist |
Hip |
Thigh |
Calf/shin |
Knee |
Ankle |
Foot/toes |
Hand/fingers |
Explain ALL checked answers (include dates):__________________________________________
_______________________________________________________________________________
_______________________________________________________________________________
14.Have you ever had a condition/injury that required x-rays, MRI, CT scan, or therapy? Yes No If yes, explain:____________________________________________________________________
15.Do you use any special equipment (braces, pads, mouthguards, neck rolls, etc.)? Yes No If yes, explain:____________________________________________________________________
16.Have you had any problems with your vision or injuries to your eyes? |
Yes |
No |
Do you wear glasses, corrective lenses, or protective eyewear? |
Yes |
No |
Explain ALL yes answers:___________________________________________________________
17.Have you ever had any skin problems (rashes, itching, MRSA, herpes, acne)?Yes No If yes, explain:____________________________________________________________________
18.Have you ever had an eating disorder or restricted food to lose weight? |
Yes |
No |
Do you want to weigh MORE or LESS than you do now? |
Yes |
No |
Do you feel stressed? |
Yes |
No |
Explain ALL yes answers:___________________________________________________________
20.FEMALES ONLY Age at 1st menstrual period?___________ Date of most recent?____________
Number of periods in the last 12 months?________ Longest time between periods?__________
21.Has a doctor ever denied or restricted your participation in sports for any reason? Yes No If yes, explain;____________________________________________________________________
**I hereby state that, to the best of my knowledge, the answers to the above questions are complete and correct.
Signature of Athlete:_____________________________________________ Date:_____________
Signature of Parent/Guardian:______________________________________ Date:____________