
CHP-500 can be filled in online without difficulty. Just try FormsPal PDF editor to complete the task in a timely fashion. Our development team is always working to develop the editor and insure that it is much easier for users with its cutting-edge functions. Bring your experience to another level with continuously improving and exciting options we offer! Here's what you'd want to do to start:
Step 1: Hit the "Get Form" button at the top of this page to access our tool.
Step 2: As soon as you open the tool, you'll see the form made ready to be filled in. Other than filling in different fields, you could also perform various other actions with the form, that is adding custom text, changing the initial textual content, inserting images, putting your signature on the form, and a lot more.
To be able to fill out this document, ensure you type in the necessary details in each and every blank:
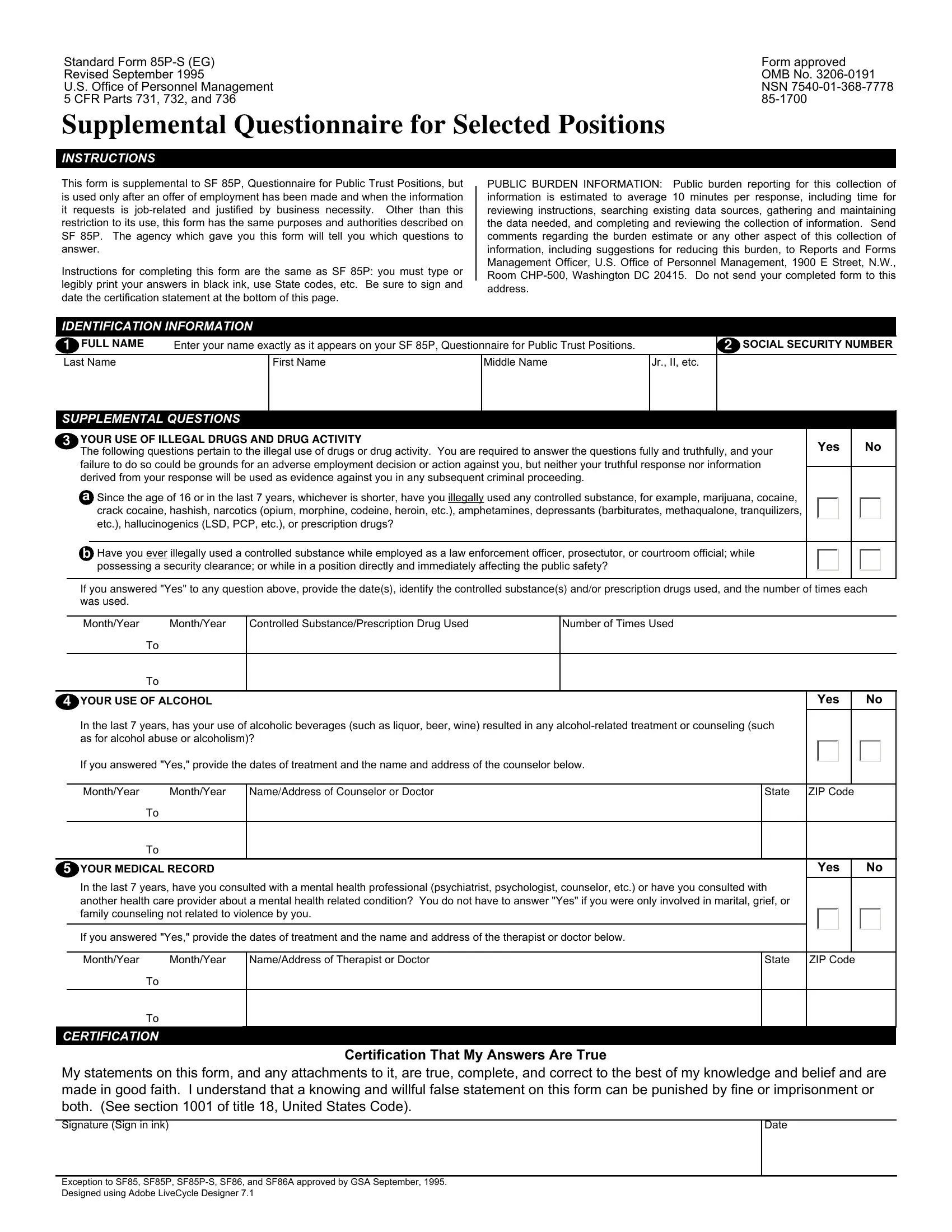
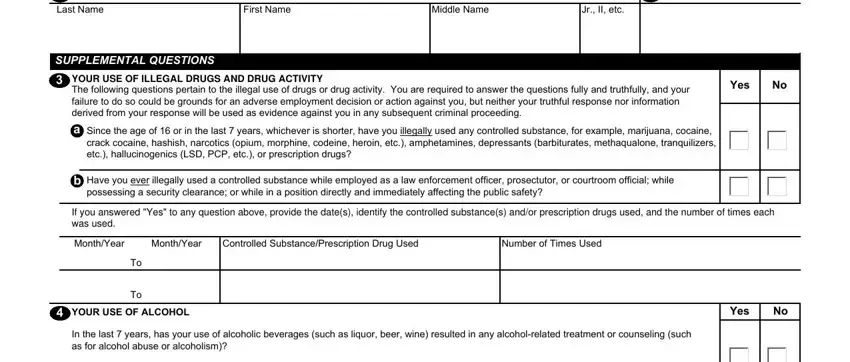
1. Start completing your CHP-500 with a group of necessary fields. Consider all of the required information and make certain there is nothing left out!
2. Immediately after the first part is filled out, proceed to enter the applicable information in all these - MonthYear MonthYear, NameAddress of Counselor or Doctor, State, ZIP Code, YOUR MEDICAL RECORD, Yes, In the last years have you, If you answered Yes provide the, MonthYear MonthYear, NameAddress of Therapist or Doctor, State, ZIP Code, CERTIFICATION, My statements on this form and any, and Date.
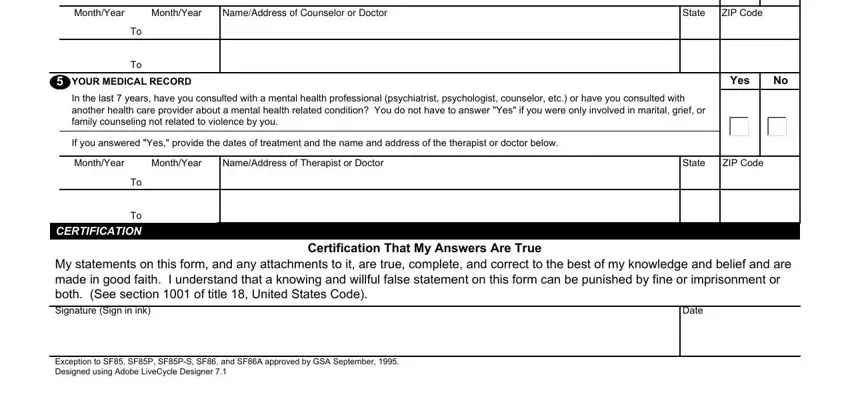
Be very mindful when filling out ZIP Code and Date, as this is where most users make mistakes.
Step 3: Confirm that your details are correct and simply click "Done" to finish the task. Right after starting afree trial account at FormsPal, you will be able to download CHP-500 or send it through email without delay. The PDF form will also be accessible from your personal account page with your changes. We do not share any details you use whenever filling out forms at our site.