


State Form 43202 can be filled in with ease. Just try FormsPal PDF tool to do the job without delay. In order to make our editor better and simpler to utilize, we consistently develop new features, taking into account suggestions coming from our users. If you are looking to start, here is what it will take:
Step 1: Access the PDF form inside our editor by clicking the "Get Form Button" at the top of this page.
Step 2: Using this online PDF tool, you could accomplish more than just fill in blank form fields. Try all the features and make your forms appear professional with customized textual content put in, or optimize the file's original content to perfection - all comes with the capability to incorporate any graphics and sign the document off.
This form requires specific information to be filled in, therefore be sure you take whatever time to type in what is expected:
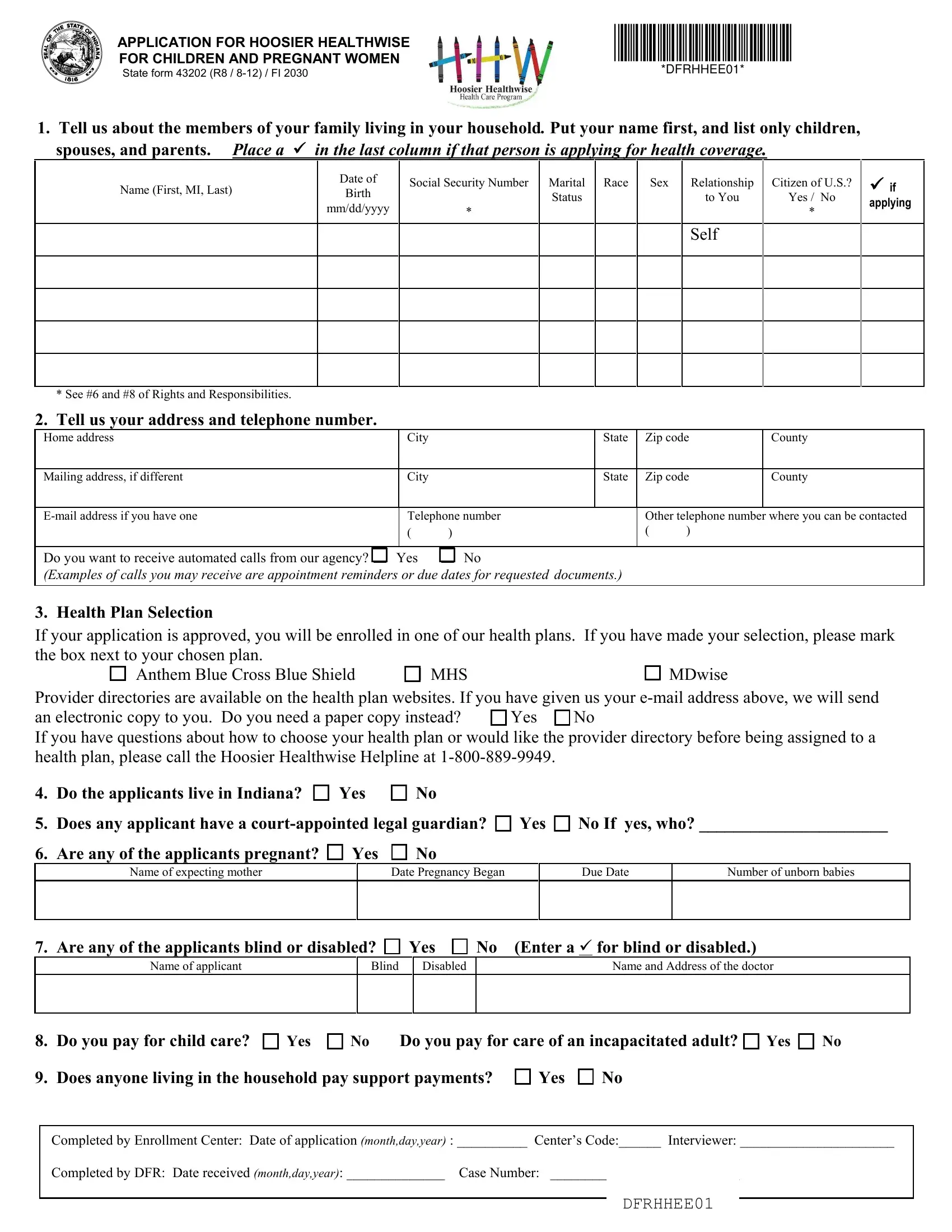
1. Start filling out the State Form 43202 with a number of major blanks. Consider all of the required information and be sure there is nothing missed!
2. After the last segment is completed, you're ready put in the required specifics in Health Plan Selection If your, Does any applicant have a, Are any of the applicants, Name of expecting mother, Date Pregnancy Began, Due Date, Number of unborn babies, Are any of the applicants blind, Name of applicant, Blind, Disabled, Name and Address of the doctor, and Do you pay for child care Yes in order to go to the 3rd step.
3. In this particular part, have a look at Are any applicants covered by, Did any applicants who do not, If yes who When did coverage end, Company ended coverage Other, Noncustodial parent dropped, Tell us how much work income you, Name of person working, Name of person working, Start Date End Date How often, Start Date End Date How often, Amount of Gross Pay Per Pay Period, Amount of Gross Pay Per Period, Is person selfemployed Yes No, Is person selfemployed Yes No, and Employer name and phone number. Each one of these will need to be filled in with greatest accuracy.
4. This next section requires some additional information. Ensure you complete all the necessary fields - income initial here For child, Military Allotment Unemployment, Interest Payments Educational, Name of the Person Receiving the, Payments, What Type from above, How Often are, When did Payments, Amount of the, Payments Received, Begin, Payments, Was the household income in the, Please read the following, and I certify under penalty of perjury - to proceed further in your process!
Lots of people generally make some errors when filling in How Often are in this area. Make sure you reread what you enter here.
Step 3: Reread everything you've inserted in the form fields and hit the "Done" button. Go for a 7-day free trial option with us and gain immediate access to State Form 43202 - downloadable, emailable, and editable in your personal cabinet. At FormsPal, we do everything we can to be certain that all of your details are stored secure.