 Vision - 391.41 (b) (10)
Vision - 391.41 (b) (10)
 Hearing - 391.41 (b)(11)
Hearing - 391.41 (b)(11)

 Laboratory & Other Test Finding
Laboratory & Other Test Finding
The entire process of completing the indiana cdl physical forms is pretty hassle-free. Our experts made certain our PDF editor is not hard to use and can help prepare any form without delay. Have a look at the four steps you will need to take:
Step 1: Click the button "Get form here" to open it.
Step 2: Once you've got accessed the editing page indiana cdl physical forms, you'll be able to notice every one of the actions intended for the form in the top menu.
You will have to provide the following data to fill out the file:
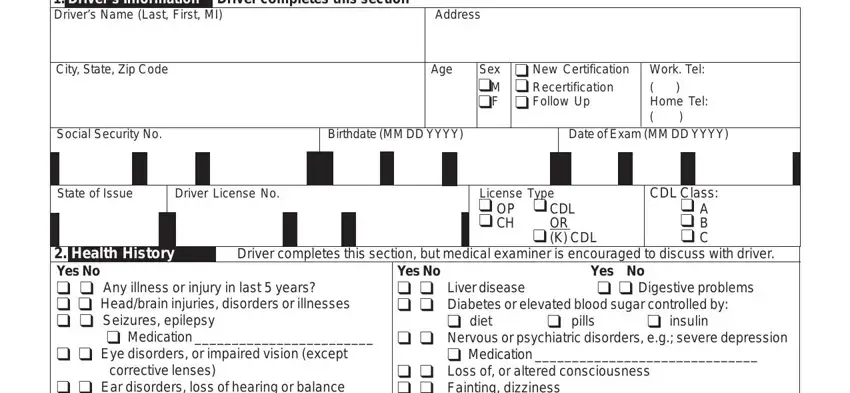
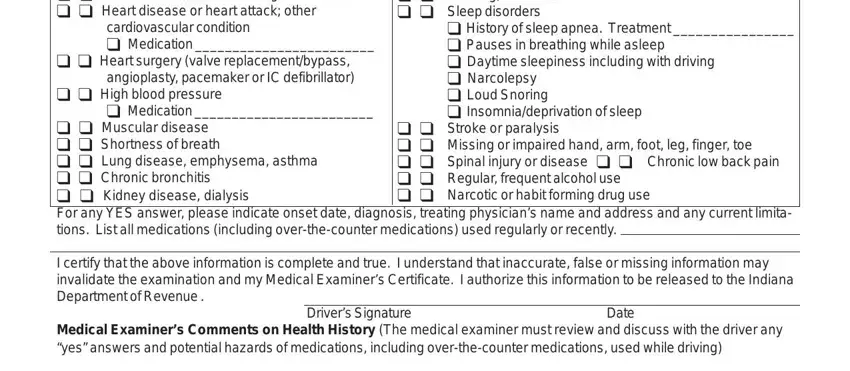
Fill in the cid cid Ear disorders loss of, cardiovascular condition cid, cid cid Heart surgery valve, cid cid High blood pressure, cid Medication, cid cid Loss of or altered, cid History of sleep apnea, cid cid Muscular disease cid cid, cid cid Stroke or paralysis cid, I certify that the above, Medical Examiners Comments on, Drivers Signature, and Date areas with any content that is demanded by the program.
In the CDLPHY Page of, and American LegalNet Inc field, describe the relevant particulars.

The Drivers Name, Testing Medical Examiner completes, Vision b Standard At least, Horizontal Field of Vision, Complete this section if vision, Acuity Uncorrected Corrected, Right Eye Left Eye Both Eyes, Applicant can recognize and, Right Eye Left Eye, cid Yes cid No, cid Corective Lenses cid Yes cid No, Date of Examination, Telephone No, Name of Ophthalmologist or, and Signature field could be used to point out the rights and responsibilities of both sides.
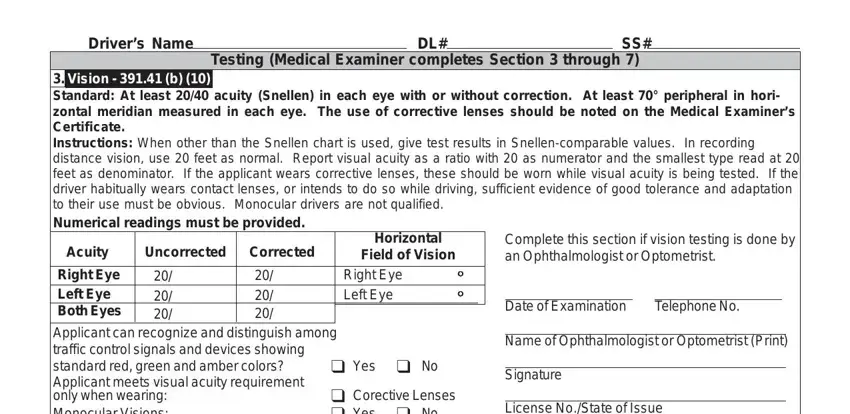
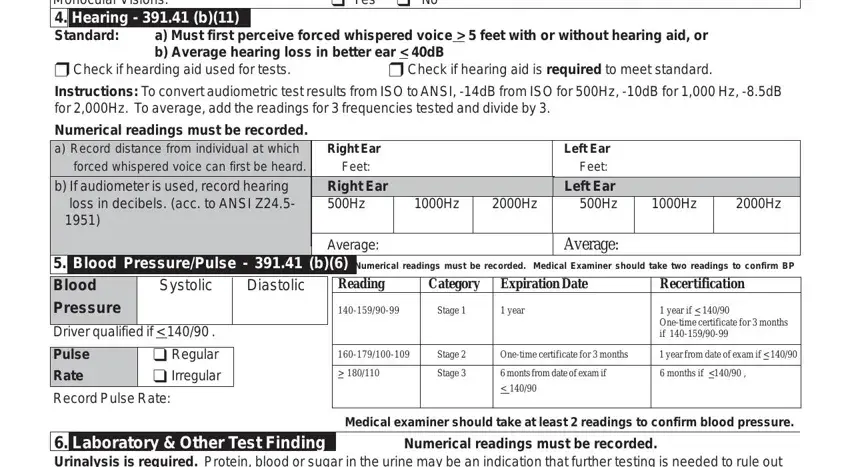
Look at the sections Applicant can recognize and, cid Corective Lenses cid Yes cid No, License NoState of Issue, a Must first perceive forced, cid Check if hearding aid used for, cid Check if hearing aid is, Numerical readings must be, Right Ear Feet Right Ear Hz, Average, Left Ear Feet Left Ear Hz, Average, Blood PressurePulse b Numerical, Expiration Date, Recertification, and Diastolic and then fill them in.
Step 3: Once you've clicked the Done button, your document is going to be readily available export to every device or email you specify.
Step 4: To protect yourself from all of the troubles later on, you will need to have a minimum of several duplicates of the document.
