
Working with PDF documents online is actually a piece of cake with our PDF tool. You can fill in sample religious exemption letter indiana here with no trouble. To maintain our editor on the cutting edge of efficiency, we strive to put into practice user-driven features and improvements on a regular basis. We're at all times looking for feedback - join us in revampimg PDF editing. In case you are seeking to get going, here is what it requires:
Step 1: Press the orange "Get Form" button above. It's going to open up our tool so that you can start filling out your form.
Step 2: Once you open the editor, you will see the form all set to be completed. Aside from filling out different fields, you can also perform other actions with the file, particularly adding your own words, changing the original text, inserting illustrations or photos, putting your signature on the PDF, and more.
This PDF doc requires specific information; to ensure correctness, remember to pay attention to the tips further down:
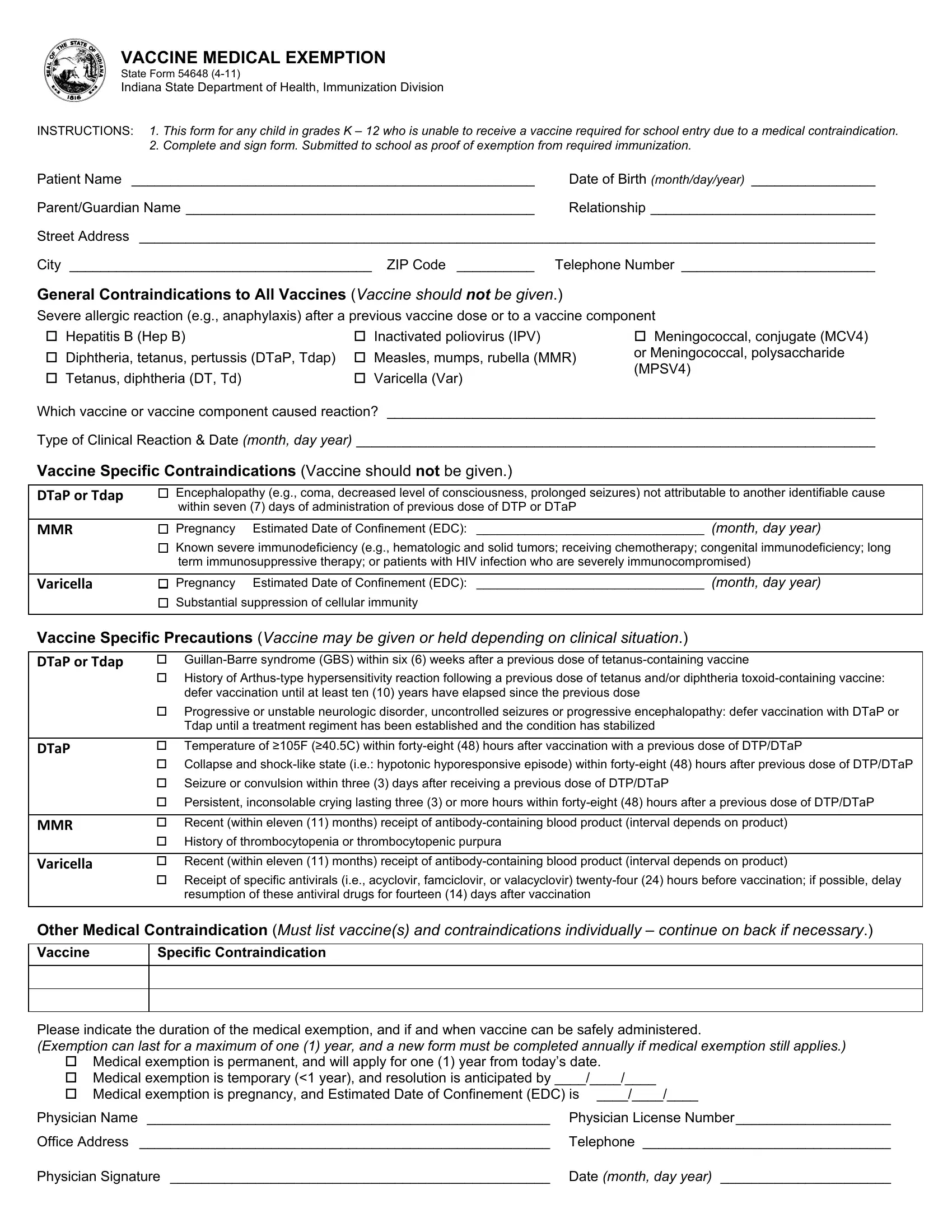
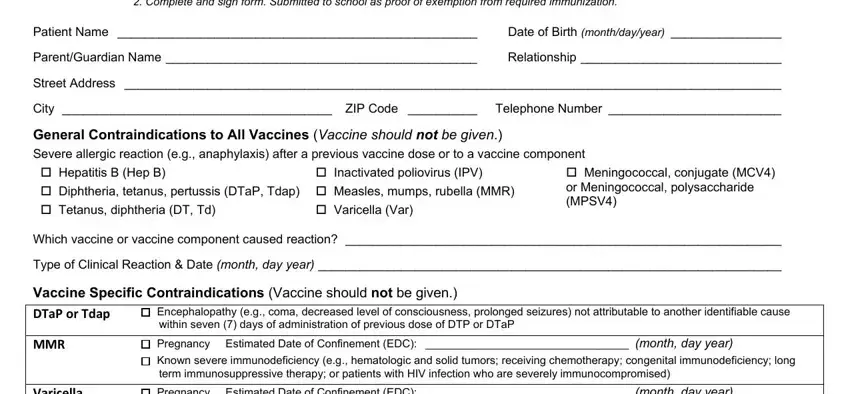
1. For starters, once completing the sample religious exemption letter indiana, start with the form section containing subsequent fields:
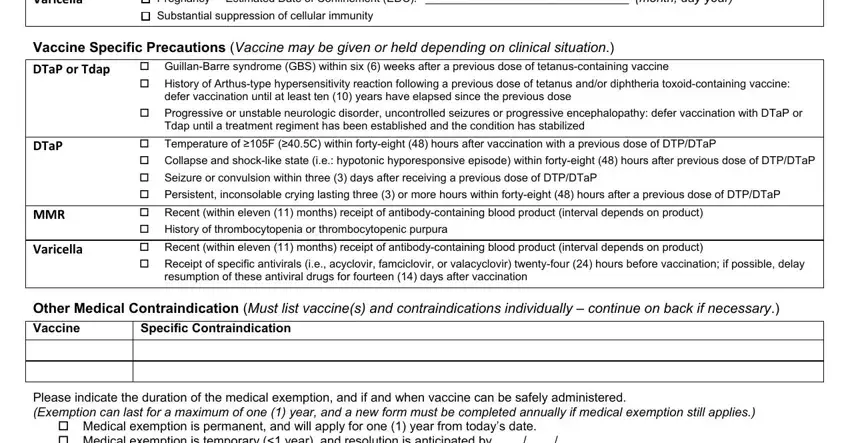
2. Now that this array of fields is done, you're ready put in the essential particulars in Varicella, Pregnancy Estimated Date of, Substantial suppression of, Vaccine Specific Precautions, cid GuillanBarre syndrome GBS, defer vaccination until at least, DTaP, MMR, Varicella, cid Progressive or unstable, Tdap until a treatment regiment, cid Temperature of F C within, resumption of these antiviral, Other Medical Contraindication, and Vaccine so you can move forward further.
As to DTaP and Varicella, be sure you do everything correctly here. These two are the most important ones in the page.
3. This third step will be straightforward - fill in every one of the form fields in cid Medical exemption is permanent, Physician Name Physician License, Office Address Telephone, and Physician Signature Date month in order to complete the current step.

Step 3: Ensure that your information is correct and press "Done" to continue further. Sign up with us now and easily gain access to sample religious exemption letter indiana, set for download. All changes you make are preserved , letting you edit the file at a later stage when required. When you use FormsPal, you can fill out documents without worrying about database leaks or data entries getting shared. Our protected software makes sure that your personal data is maintained safe.