
Whenever you desire to fill out pennsylvania statement of claim request form, you don't have to install any applications - simply try using our online tool. The editor is continually maintained by our staff, getting handy features and becoming greater. To get the ball rolling, go through these simple steps:
Step 1: Open the PDF file inside our tool by hitting the "Get Form Button" at the top of this page.
Step 2: The editor will let you customize your PDF form in many different ways. Improve it by writing customized text, correct existing content, and include a signature - all readily available!
In order to finalize this document, ensure that you provide the information you need in each and every field:
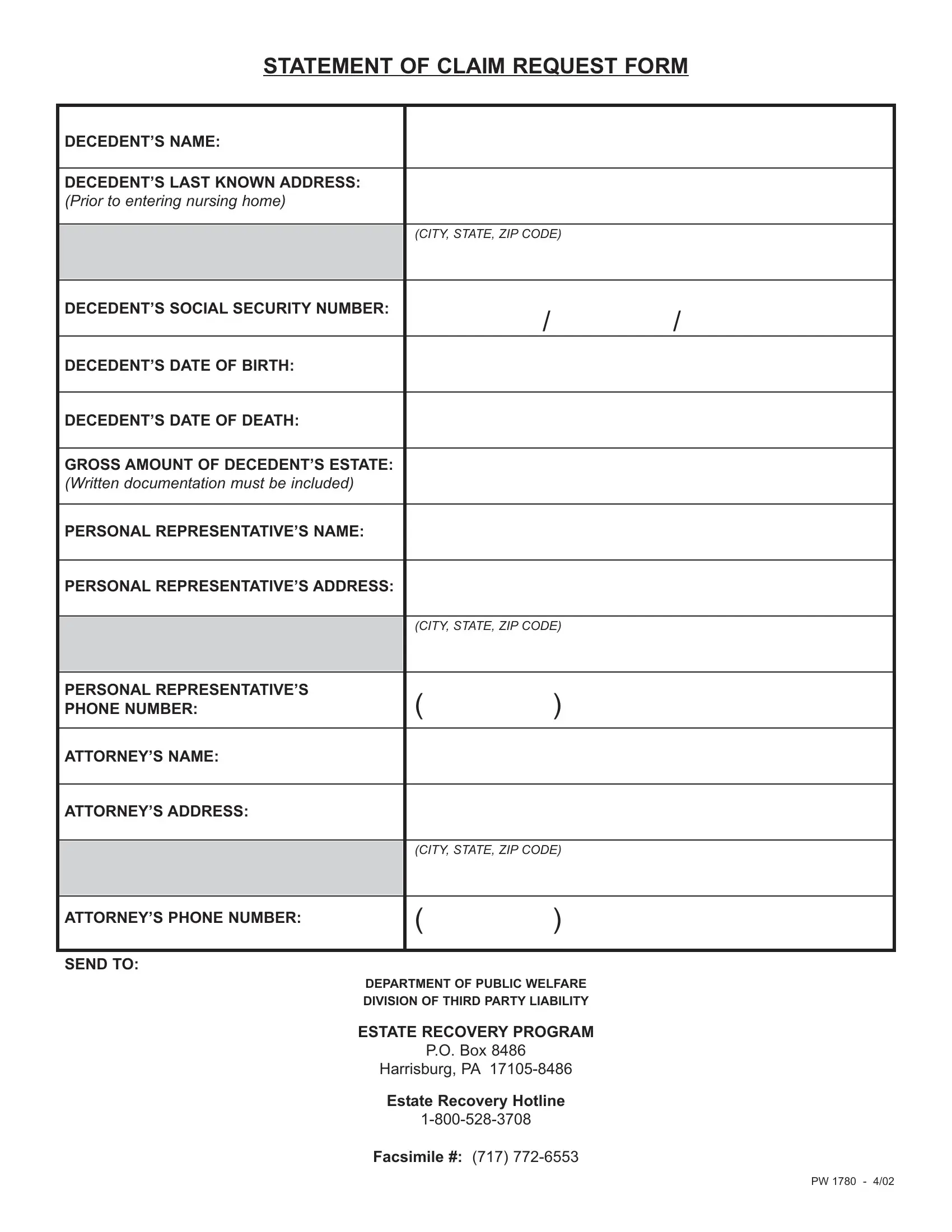
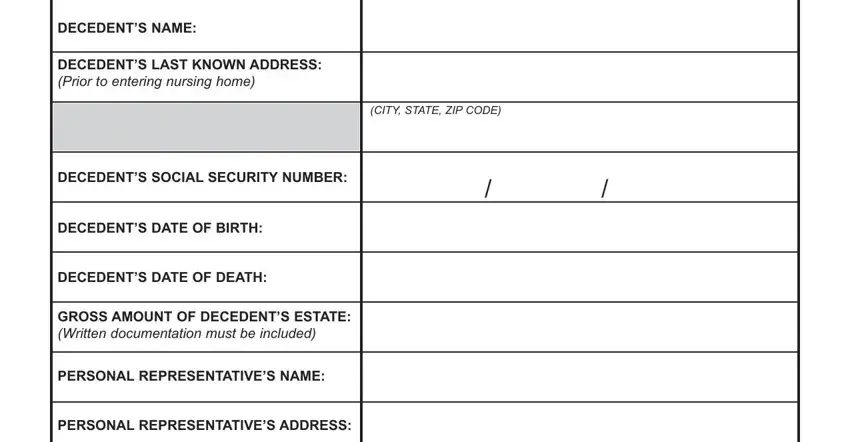
1. The pennsylvania statement of claim request form usually requires specific information to be inserted. Make sure the subsequent blanks are completed:
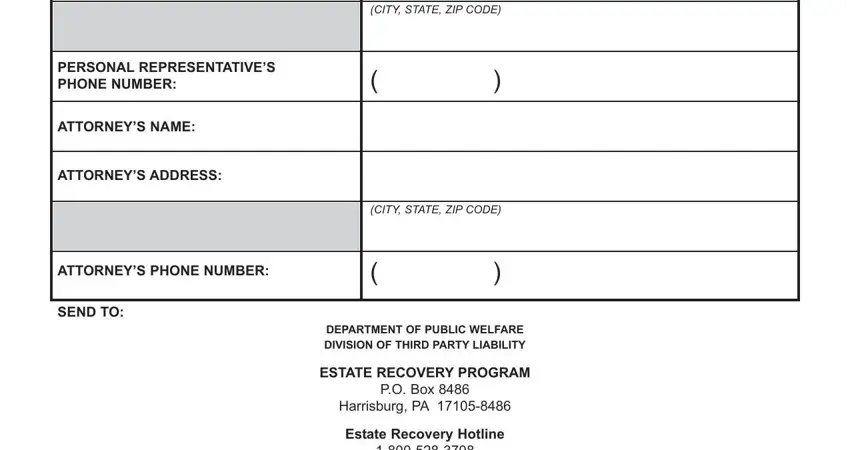
2. Once your current task is complete, take the next step – fill out all of these fields - CITY STATE ZIP CODE, PERSONAL REPRESENTATIVES PHONE, ATTORNEYS NAME, ATTORNEYS ADDRESS, CITY STATE ZIP CODE, ATTORNEYS PHONE NUMBER, SEND TO, DEPARTMENT OF PUBLIC WELFARE, ESTATE RECOVERY PROGRAM, PO Box, Harrisburg PA, and Estate Recovery Hotline with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
It's very easy to get it wrong when completing the DEPARTMENT OF PUBLIC WELFARE, so ensure that you take another look before you finalize the form.
Step 3: Immediately after looking through your filled out blanks, click "Done" and you are all set! Right after starting afree trial account with us, you'll be able to download pennsylvania statement of claim request form or send it via email right away. The PDF will also be readily accessible from your personal account menu with all of your modifications. When you work with FormsPal, you can fill out documents without the need to worry about personal information leaks or records being distributed. Our secure software helps to ensure that your private data is stored safe.