
Should you need to fill out student emergency card, you don't have to install any programs - simply try using our PDF editor. Our tool is consistently evolving to give the very best user experience attainable, and that's due to our commitment to constant improvement and listening closely to feedback from users. Here is what you will want to do to get going:
Step 1: Click the orange "Get Form" button above. It is going to open up our tool so you can start completing your form.
Step 2: The editor will give you the opportunity to customize PDF forms in a range of ways. Change it with your own text, correct what is already in the document, and place in a signature - all within a couple of mouse clicks!
It will be an easy task to complete the pdf adhering to this helpful tutorial! This is what you have to do:
1. While completing the student emergency card, be certain to complete all of the important blanks in its corresponding part. It will help to expedite the work, which allows your details to be processed swiftly and appropriately.
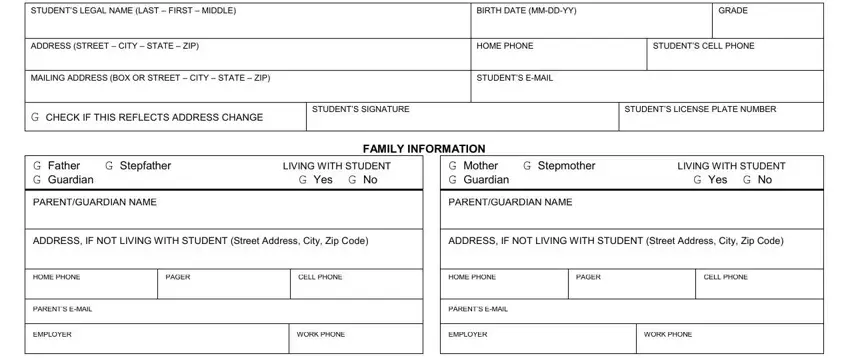
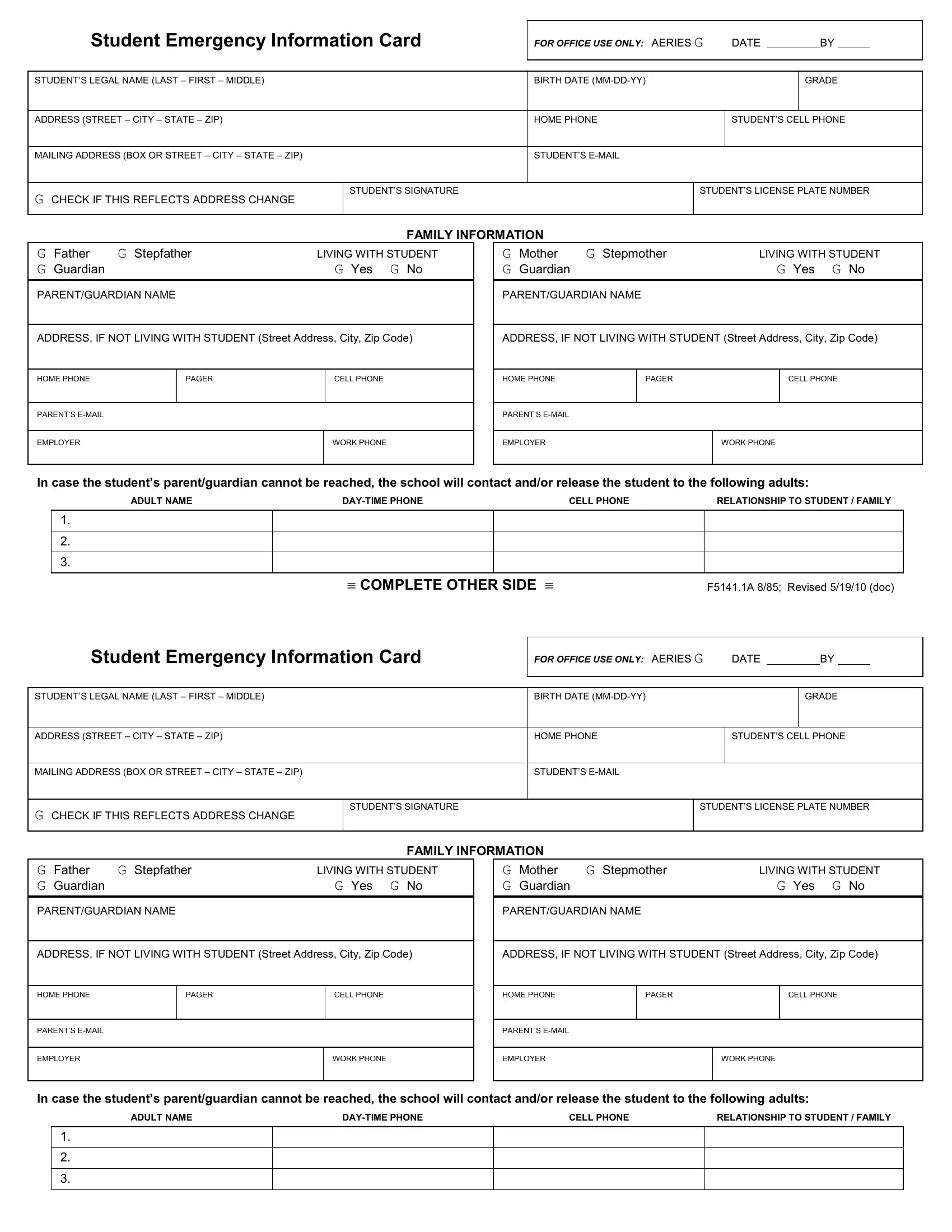
2. Your next step would be to fill out the next few fields: In case the students, ADULT NAME, DAYTIME PHONE, CELL PHONE, RELATIONSHIP TO STUDENT FAMILY, COMPLETE OTHER SIDE FA Revised, Student Emergency Information Card, FOR OFFICE USE ONLY AERIES G DATE, STUDENTS LEGAL NAME LAST FIRST, G CHECK IF THIS REFLECTS ADDRESS, BIRTH DATE MMDDYY, HOME PHONE, STUDENTS EMAIL, STUDENTS SIGNATURE, and FAMILY INFORMATION.
Be extremely attentive when filling out Student Emergency Information Card and STUDENTS SIGNATURE, because this is the part in which most users make errors.
3. Completing PARENTGUARDIAN NAME, PARENTGUARDIAN NAME, ADDRESS IF NOT LIVING WITH STUDENT, ADDRESS IF NOT LIVING WITH STUDENT, HOME PHONE, PAGER, CELL PHONE, HOME PHONE, PAGER, CELL PHONE, PARENTS EMAIL, EMPLOYER, WORK PHONE, PARENTS EMAIL, and EMPLOYER is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. This next section requires some additional information. Ensure you complete all the necessary fields - Siblings, Name, Name, Name, Age, Age, Age, School, School, School, MEDICAL INFORMATION please check, Allergic Reactions, G Yes, G No, and If yes type of allergies - to proceed further in your process!
5. Now, this last part is what you should finish before finalizing the form. The blank fields at issue are the next: Siblings, Name, Name, Name, Age, Age, Age, School, School, School, MEDICAL INFORMATION please check, Allergic Reactions, G Yes, G No, and If yes type of allergies.
Step 3: Immediately after taking another look at the completed blanks, hit "Done" and you're all set! After registering afree trial account with us, you will be able to download student emergency card or email it right away. The PDF document will also be at your disposal in your personal cabinet with your each edit. FormsPal guarantees secure form completion with no personal information recording or sharing. Rest assured that your information is secure with us!