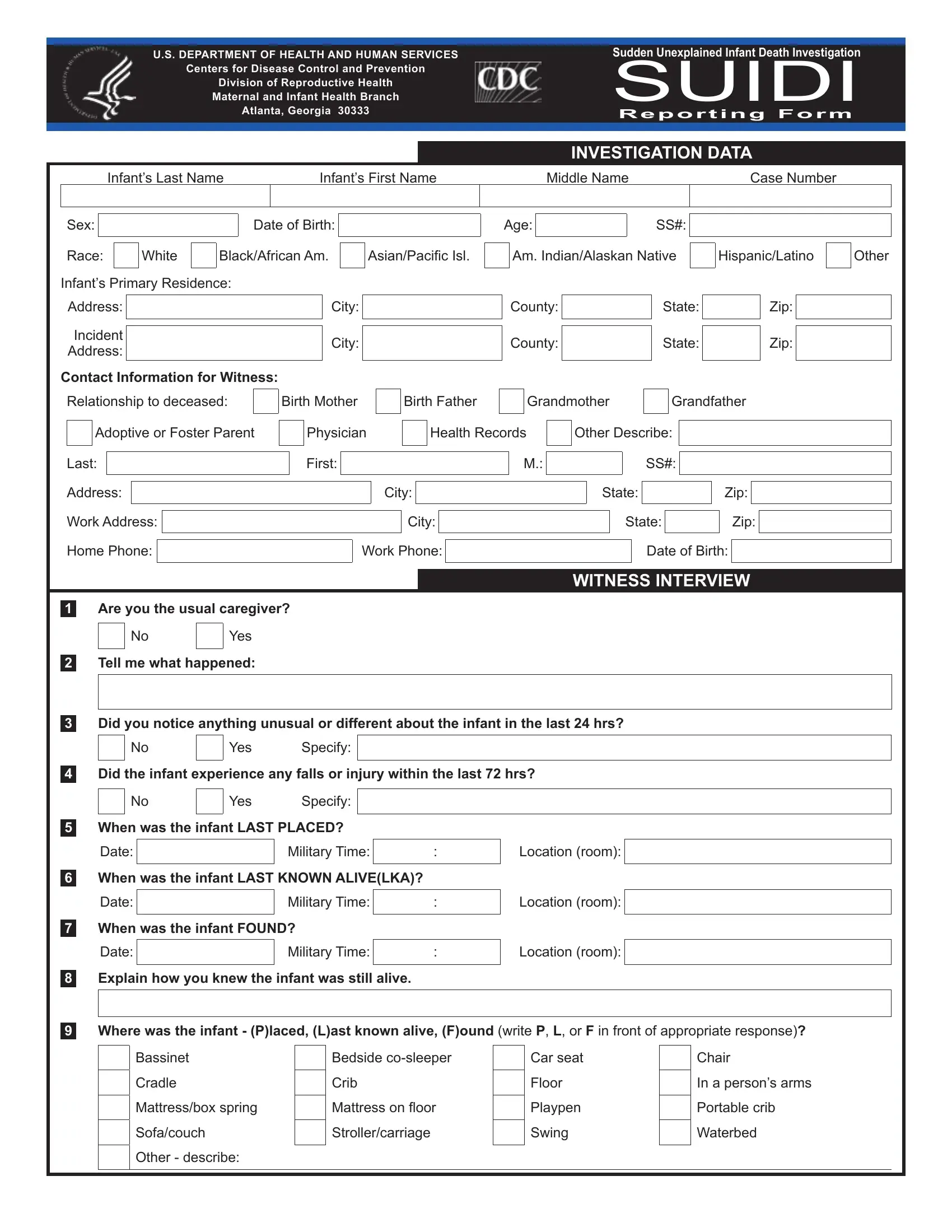
Understanding the critical aspects of the Sudden Unexplained Infant Death Investigation (SUIDI) Reporting Form, curated by the U.S. Department of Health and Human Services, specifically the Centers for Disease Control and Prevention’s Division of Reproductive Health, is imperative for those involved in post-infant death investigations. The form serves a multifaceted purpose, acting both as a thorough data collection tool and a significant resource for health professionals to analyze and prevent future incidents. By meticulously gathering details such as the infant's sleeping environment, including bedding and sleeping position, alongside potential risk factors like exposure to smoke or the infant's dietary history, this document encapsulates a broad spectrum of variables. Additionally, it encompasses witness interviews, infant medical and dietary histories, and intricate aspects of the death scene investigation. This comprehensive approach not only aids in elucidating the circumstances surrounding an infant's unexpected death but also garners valuable insights for ongoing research in the prevention of such distressing occurrences. With sections dedicated to the investigation data, witness interviews, and detailed accounts of the infant's health, the form is a cornerstone in the strategic framework designed to combat the enigma of sudden infant deaths.
| Question | Answer |
|---|---|
| Form Name | Suidi Reporting Form |
| Form Length | 8 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min |
| Other names | cdc suidirf, suidi reporting form, death reporting form, sudden death form |
|
|
|
|
|
|
|
|
|
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES |
Sudden Unexplained Infant Death Investigation |
|||||
|
Centers for Disease Control and Prevention |
SUIDI |
|||||
|
|
|
|
||||
|
Division of Reproductive Health |
|
|
|
|||
|
Maternal and Infant Health Branch |
|
|
|
|||
|
|
Atlanta, Georgia 30333 |
Reporting Form |
||||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
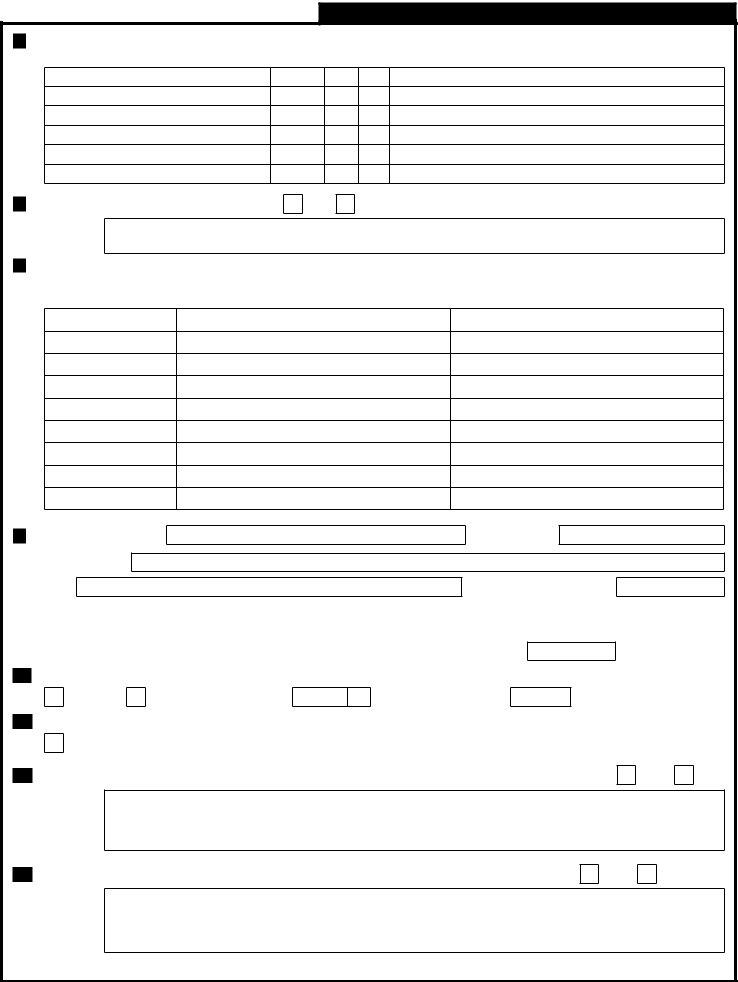
INVESTIGATION DATA |
||
|
Infant’s Last Name |
|
Infant’s First Name |
Middle Name |
Case Number |
||
|
|
|
|
|
|
|
|
Sex:
Race:
White
Date of Birth:
Black/African Am.
Asian/Paciic Isl.
Age: |
|
SS#: |
|
|
|
Am. Indian/Alaskan Native
Hispanic/Latino
Other
Infant’s Primary Residence: Address:
Incident
Address:
Contact Information for Witness:
City:
City:
County:
County:
State:
State:
Zip:
Zip:
Relationship to deceased: |
|
Birth Mother |
|
Birth Father |
|
|
|
Grandmother |
|
|
Grandfather |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Adoptive or Foster Parent |
|
|
Physician |
|
|
|
Health Records |
|
|
Other Describe: |
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Last: |
|
|
|
|
|
|
First: |
|
|
|
|
|
|
|
|
|
|
M.: |
|
|
|
|
|
|
SS#: |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Address: |
|
|
|
|
|
|
|
|
|
City: |
|
|
|
|
|
|
|
|
|
State: |
|
|
|
|
|
|
Zip: |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
Work Address: |
|
|
|
|
|
|
|
|
City: |
|
|
|
|
|
|
|
|
|
|
State: |
|
|
|
|
Zip: |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
Home Phone: |
|
|
|
|
|
Work Phone: |
|
|
|
|
|
|
|
|
|
|
|
|
Date of Birth: |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
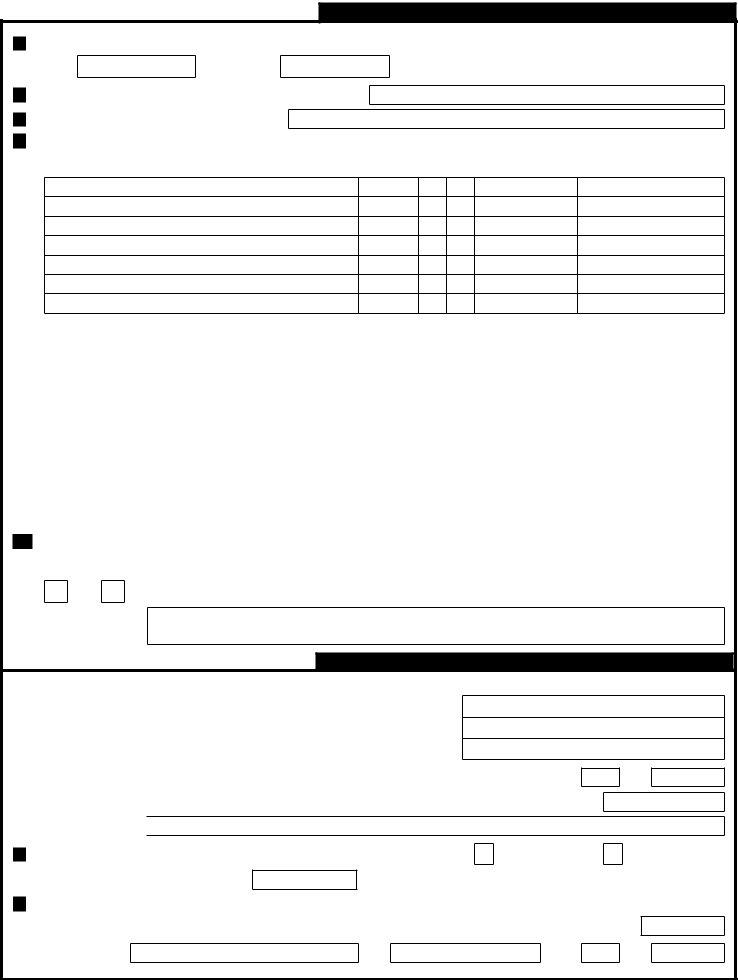
WITNESS INTERVIEW
1Are you the usual caregiver?
No
Yes
2Tell me what happened:
3Did you notice anything unusual or different about the infant in the last 24 hrs?
No |
|
Yes |
Specify: |
|
|
|
|
4Did the infant experience any falls or injury within the last 72 hrs?
No
Yes Specify:
5When was the infant LAST PLACED?
Date: |
|
Military Time: |
|
|
|
6When was the infant LAST KNOWN ALIVE(LKA)?
Date: |
|
Military Time: |
|
|
|
7When was the infant FOUND?
WITNESS INTERVIEW (cont.)
10In what position was the infant LAST PLACED? Was this the infant’s usual position?
11In what position was the infant LKA? Was this the infant’s usual position?
12In what position was the infant FOUND? Was this the infant’s usual position?
Sitting
Yes
Sitting
Yes
Sitting
Yes
On back |
On side |
On stomach |
No |
What was the usual position? |
|
On back |
On side |
On stomach |
No |
What was the usual position? |
|
On back |
On side |
On stomach |
No |
What was the usual position? |
|
Unknown
Unknown
Unknown
13 |
Face position when LAST PLACED? |
Face down on surface |
Face up |
Face right |
Face left |
|||||||
|
|
|
|
|
|
|
|
|||||
14 |
Neck position when LAST PLACED? |
Hyperextended (head back) |
Flexed (chin to chest) |
Neutral |
Turned |
|||||||
|
|
|
|
|
|
|
|
|
|
|
||
15 |
Face position when LKA? |
Face down on surface |
|
Face up |
|
Face right |
|
Face left |
|
|
||
|
|
|
|
|
|
|
|
|
||||
16 |
Neck position when LKA? |
Hyperextended (head back) |
Flexed (chin to chest) |
Neutral |
|
Turned |
||||||
|
|
|
|
|
|
|
|
|
|
|
||
17 |
Face position when FOUND? |
Face down on surface |
|
Face up |
|
Face right |
|
Face left |
|
|
||
|
|
|
|
|
|
|
|
|
||||
18 |
Neck position when FOUND? |
Hyperextended (head back) |
Flexed (chin to chest) |
Neutral |
|
Turned |
||||||
|
|
|
|
|
|
|
|
|
|
|||
19 |
What was the infant wearing? (ex. |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
20 |
Was the infant tightly wrapped or swaddled? |
No |
Yes - describe: |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
21Please indicate the types and numbers of layers of bedding both over and under infant (not including wrapping blanket):
Bedding UNDER Infant |
None |
Number Bedding OVER Infant |
None |
Number |
|
Receiving blankets |
|
|
Receiving blankets |
|
|
|
|
|
|
|
|
Infant/child blankets |
|
|
Infant/child blankets |
|
|
|
|
|
|
|
|
Infant/child comforters (thick) |
|
|
Infant/child comforters (thick) |
|
|
|
|
|
|
|
|
Adult comforters/duvets |
|
|
Adult comforters/duvets |
|
|
|
|
|
|
|
|
Adult blankets |
|
|
Adult blankets |
|
|
|
|
|
|
|
|
Sheets |
|
|
Sheets |
|
|
|
|
|
|
|
|
Sheepskin |
|
|
Pillows |
|
|
|
|
|
|
|
|
Pillows |
|
|
Other, specify: |
|
|
|
|
|
|
|
|
Rubber or plastic sheet |
|
|
|
|
|
|
|
|
|
|
|
Other, specify: |
|
|
|
|
|
|
|
|
|
|
|
22Which of the following devices were operating in the infant’s room?
|
|
|
None |
|
Apnea monitor |
|
Humidiier |
|
Vaporizer |
|
Air puriier |
||
|
|
|
|
|
|
|
|
||||||
23 |
In was the temperature in the infant’s room? |
|
|
Hot |
|
Cold |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
24Which of the following items were near the infant’s face, nose, or mouth?
Other - |
|
Normal |
Other - |
Bumper pads
Infant pillows
Positional supports
Stuffed animals
Toys
Other -
25Which of the following items were within the infant’s reach?
|
|
|
Blankets |
|
Toys |
|
Pillows |
|
|
Paciier |
|
|
Nothing |
||
|
|
|
|
|
|
|
|||||||||
26 |
Was anyone sleeping with the infant? |
|
|
No |
|
Yes |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other -
|
|
|
|
Location in relation |
|
Name of individual sleeping with infant Age |
Height Weight |
to infant |
Imparement (intoxication, tired) |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
27 |
Was there evidence of wedging? |
|
No |
|
|
Yes - Describe: |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
28 |
When the infant was found, was s/he: |
|
|
Breathing |
|
|
Not Breathing |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If not breathing, did you witness the infant stop breathing? |
|
|
|
No |
|
|
Yes |
||||||
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page 2
WITNESS INTERVIEW (cont.)
29What had led you to check on the infant?
30Describe the infant’s appearance when found.
Appearance |
Unknown No Yes |
Describe and specify location |
a)Discoloration around face/nose/mouth
b)Secretions (foam, froth)
c)Skin discoloration (livor mortis)
d)Pressure marks (pale areas, blanching)
e)Rash or petechiae (small, red blood spots on skin, membranes, or eyes)
f)Marks on body (scratches or bruises)
g)Other
31
32
33
What did the infant feel like when found? (Check all that apply.) |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
Sweaty |
|
Warm to touch |
|
Cool to touch |
|
Limp, lexible |
|
|
Rigid, stif |
|
Unknown |
|
|||||||||
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Other - specify: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Did anyone else other than EMS try to resuscitate the infant? |
|
No |
|
|
|
Yes |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Who? |
|
|
|
|
|
|
|
Date: |
|
|
|
|
|
|
|
Military time: |
|
: |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please describe what was done as part of resuscitation:
34Has the parent/caregiver ever had a child die suddenly and unexpectedly? Explain:
No
Yes
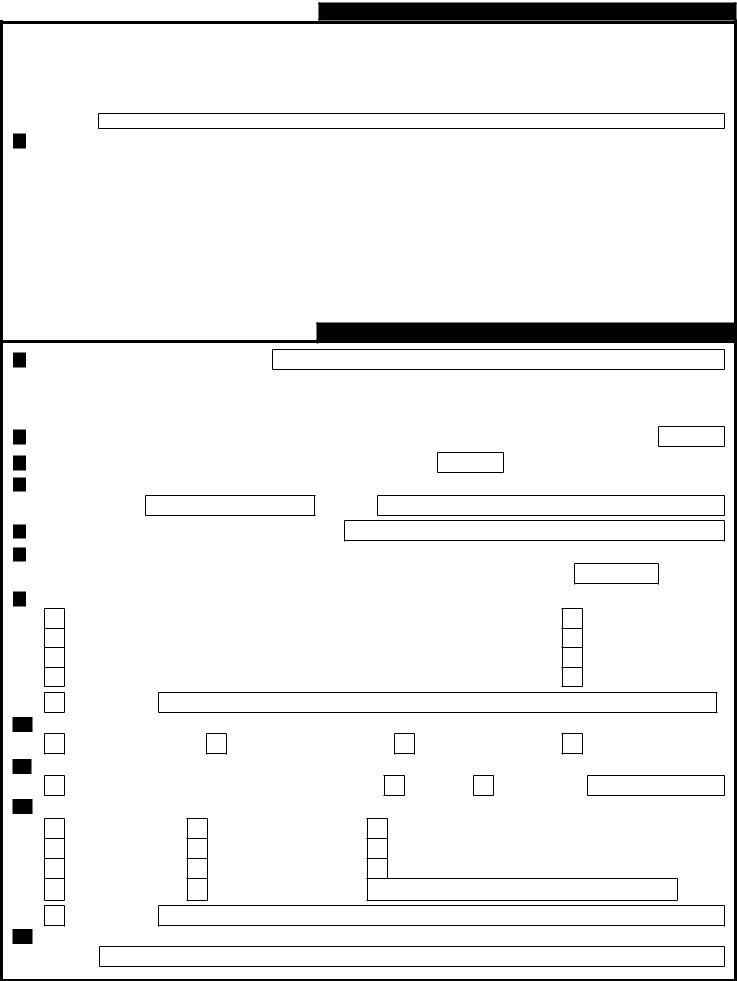
INFANT MEDICAL HISTORY
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
Source of medical information: |
|
Doctor |
|
Other healthcare provider |
|
Medical record |
|
Family |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mother/primary caregiver |
|
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2In the 72 hours prior to death, did the infant have:
Condition |
Unknown No Yes Condition |
Unknown No Yes |
|||||||
|
|
|
|
|
|
|
|
|
|
a) Fever |
|
|
|
k) |
Apnea (stopped breathing) |
|
|
|
|
h) Diarrhea |
|
|
|
e) |
Decrease in appetite |
|
|
|
|
b) Excessive sweating |
|
|
|
l) |
Cyanosis (turned blue/gray) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
i) |
Stool changes |
|
|
|
f) |
Vomiting |
|
|
|
|
|
|
|
|
|
|
|
|
|
c) |
Lethargy or sleeping more than usual |
|
|
|
m) Seizures or convulsions |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
j) |
Dificulty breathing |
|
|
|
g) Choking |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d) |
Fussiness or excessive crying |
|
|
|
n) Other, specify: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3In the 72 hours prior to death, was the infant injured or did s/he have any other condition(s) not mentioned?
|
|
|
No |
|
Yes - describe: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
4 |
|
In the 72 hours prior to the infants death, was the infant given any vaccinations or medications? |
|
No |
|
Yes |
||||
(Please include any home remedies, herbal medications, prescription medicines,
|
|
Date given |
|
Approx. time |
|
||
|
|
|
|
|
|
|
|
Name of vaccination or medication |
Dose last given Month Day |
Year |
(Military Time) |
comments: |
|||
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page 3
INFANT MEDICAL HISTORY (cont.)
5At any time in the infant’s life, did s/he have a history of?
Medical history |
Unknown No Yes |
Describe |
a)Allergies (food, medication, or other)
b)Abnormal growth or weight gain/loss
c)Apnea (stopped breathing)
d)Cyanosis (turned blue/gray)
e)Seizures or convulsions
f)Cardiac (heart) abnormalities
6Did the infant have any birth defects(s)? Describe:
No
Yes
7Describe the two most recent times that the infant was seen by a physician or health care provider:
(Include emergency department visits, clinic visits, hospital admissions, observational stays, and telephone calls)
First most recent visit |
Second most recent visit |
a)Date
b)Reason for visit
c)Action taken
d)Physician’s name
e)Hospital/clinic
f)Address
g)City
h)State, ZIP
i)Phone number
8Birth hospital name: Street address:
City:
Discharge date:
State: |
|
Zip: |
|
|
|
|
|
|
|
|
|
|
9 |
|
What was the infant’s length at birth? |
|
inches or |
|
centimeters |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10 |
What was the infant’s weight at birth? |
|
pounds |
|
ounces or |
|
|
|
|
|
|
|
|
11Compared to the delivery date, was the infant born on time, early, or late?
grams
On time
Early - how many weeks?
Late - how many weeks?
12Was the infant a singleton, twin, triplet, or higher gestation?
Singleton |
|
Twin |
|
Triplet |
|
Quadrupelet or higher gestation |
|
|
|
|
|
|
|
13Were there any complications during delivery or at birth? (emergency
Yes
No
14Are there any alerts to the pathologist? (previous infant deaths in family, newborn screen results) Specify:
Yes
No
Page 4
INFANT DIETARY HISTORY
1On what day and at what approximate time was the infant last fed?
Date:
Military Time:
:
2 What is the name of the person who last fed the infant? 3 What is his/her relationship to the infant?
4What foods and liquids was the infant fed in the last 24 hours (include last fed)?
Food |
Unknown No Yes Quantity (ounces) Specify: (type and brand) |
a)Breast milk (one/both sides, length of time)
b)Formula (brand, water source - ex. Similac, tap water)
c)Cow’s milk
d)Water (brand, bottled, tap, well)
e)Other liquids (teas, juices)
f)Solids
g)Other
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
Was a new food introduced in the 24 hours prior to his/her death? |
|
No |
|
Yes |
|
|
|||||||||||||||
|
|
If yes, describe (ex. content, amount, change in formula, introduction of solids) |
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
6 |
|
Was the infant last placed to sleep with a bottle? |
|
|
Yes |
|
No - if no, skip to question 9 below |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
7 |
|
Was the bottle propped? (i.e., object used to hold bottle while infant feeds) |
|
|
No |
|
|
Yes |
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If yes, what object was used to prop the bottle? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
8 |
|
What was the quantity of liquid (in ounces) in the bottle? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
9 |
|
Did the death occur during? |
|
|
|
|
|
Eating solid foods |
|
Not during feeding |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10Are there any factors, circumstances, or environmental concerns that may have impacted the infant that have not yet been identiied? (ex. exposed to cigarette smoke or fumes at someone else’s home, infant unusually heavy, placed with positional supports or wedges)
No
Yes
If yes, - describe:
PREGNANCY HISTORY
1 |
Information about the infant’s birth mother: |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
First name: |
|
|
|
|
|
|
|
Last name: |
|
|
Middle name: |
|
|
|
|
|
|
Maiden name: |
||
|
|
|
|
|
|
|
||||
|
Birth date: |
|
|
|
|
|
|
|
SS#: |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Street address: |
|
|
|
City: |
|
|
|||
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|||||
|
How long has the birth mother been at this address? |
Years: |
|
|
||||||
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|||
|
Previous Address: |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
State:
Months:
Zip:
2At how many weeks or months did the birth mother begin prenatal care?
Weeks: |
|
Months: |
|
|
|
No parental care
Unknown
3Where did the birth mother receive prenatal care? (Please specify physician or other health care provider name and address.)
Physician/provider: |
|
Hospital/clinic: |
|
Phone: |
|
|
|
|
|
Street address:
City:
State:
Zip:
Page 5
PREGNANCY HISTORY (cont.)
|
|
|
|
|
|
|
|
|
|
|
4 |
At how many weeks or months did the birth mother begin prenatal care? |
|
No |
|
Yes |
|
|
|||
|
(ex. high blood pressure, bleeding, gestational diabetes) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Specify: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
5 |
Was the birth mother injured during her pregnancy with the infant? (ex. auto accident, falls) |
|
|
No |
|
Yes |
||||
|
|
|
|
|
|
|
|
|
|
|
Specify:
6During her pregnancy, did she use any of the following?
|
|
|
Unknown |
No |
Yes |
Daily |
|
Unknown |
No |
Yes |
Daily |
|
|
|
a) Over the counter medications |
|
|
|
|
|
d) Cigarettes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b) Prescription medications |
|
|
|
|
|
e) Alcohol |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c) Herbal remedies |
|
|
|
|
|
f) Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|
Currently, does any caregiver use any of the following? |
|
|
|
|
|
|
||||
|
|
|
Unknown |
No |
Yes |
Daily |
|
Unknown |
No |
Yes |
Daily |
|
|
|
a) Over the counter medications |
|
|
|
|
|
d) Cigarettes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b) Prescription medications |
|
|
|
|
|
e) Alcohol |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c) Herbal remedies |
|
|
|
|
|
f) Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INCIDENT SCENE INVESTIGATION
1Where did the incident or death occur?
|
|
|
|
|
|
|
|
|
|
2 |
Was this the primary residence? |
|
No |
|
Yes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
3 |
Is the site of the incident or death scene a daycare or other childcare setting? |
|
Yes |
|
No - If no, skip to question 8 |
||||
|
|
|
|
|
|
|
|
|
|
4How many children (under age 18) were under the care of the provider at the time of the incident or death?
5 How many adults (age 18 and over) were supervising the child(ren)?
6What is the license number and licensing agency for the daycare?
License number:
Agency:
7How long has the daycare been open for business?
8How many people live at the site of the incident or death scene?
Number of adults (18 years or older): |
|
Number of children (under 18 years old): |
|
|
|
9Which of the following heating or cooling sources were being used? (Check all that apply)
Central air |
|
Gas furnace or boiler |
|
Wood burning ireplace |
A/C window unit |
|
Electric furnace or boiler |
|
Coal burning furnace |
|
|
|||
Ceiling fan |
|
Electric space heater |
|
Kerosene space heater |
|
|
|||
Electric baseboard heat |
|
Electric (radiant) ceiling heat |
|
Window fan |
|
|
|||
|
|
|
|
|
Open window(s) Wood burning stove Floor/table fan Unknown
Thermostat setting
Thermostat reading
Actual room temp.
Outside temp.
11What was the source of drinking water at the site of the incident or death scene? (Check all that apply.)
Public/municipal water |
|
Bottled water |
|
Well |
|
|
|
|
|
12The site of the incident or death scene has: (check all that apply)
Unknown
Other - Specify:
Insects
Pets Peeling paint Rodents or vermin
Other - specify:
Mold growth
Dampness
Visible standing water
Odors or fumes - Describe:
Smoky smell (like cigarettes) Presence of alcohol containers Presence of drug paraphenalia
13Describe the general appearance of incident scene: (ex. cleanliness, hazards, overcrowding, etc.) Specify:
Page 6
INVESTIGATION SUMMARY
1Are there any factors, circumstances, or environmental concerns about the incident scene investigation that may have impacted the infant that have not yet been identiied?
2Arrival times
Law enforcement at scene:
DSI at scene:
Infant at hospital:
Military time
:
:
:
Investigator’s Notes
1Indicate the task(s) performed
|
|
|
Additional scene(s)? (forms attached) |
|
Doll reenactment/scene |
|
|
|
Photos or video taken and noted |
|||
|
|
|
Materials collected/evidence logged |
|
Referral for counseling |
|
|
|
EMS run sheet/report |
|||
|
|
|
|
|
|
|
||||||
|
|
|
Notify next of kin or verify notiication |
|
911 tape |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
2 |
|
If more than one person was interviewed, does the information differ? |
|
|
No |
|
|
Yes |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If yes, detail any differences, inconsistencies of relevant information: (ex. placed on sofa, last known alive on chair.) |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
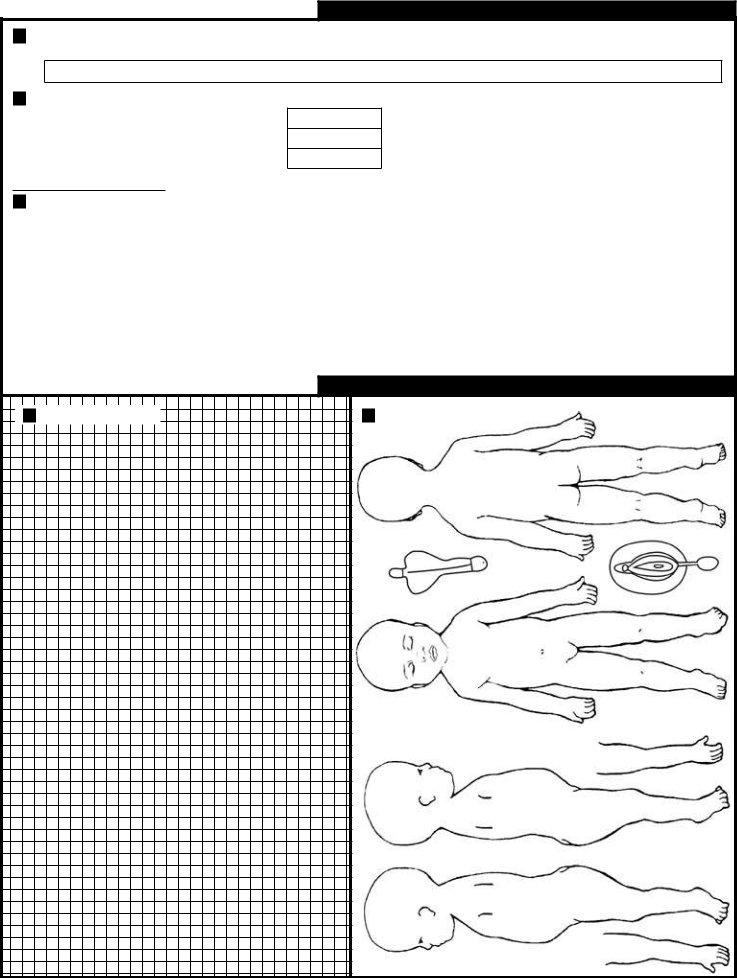
INVESTIGATION DIAGRAMS
1Scene Diagram:
2Body Diagram:
Page 7
SUMMARY FOR PATHOLOGIST
Case Information
1
2
Investigator information Name: |
|
|
|
|
|
|
|
|
Agency: |
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
Military time |
|
|
|
|
|
|
|
|
|
|||||
|
Investigated: |
|
|
|
|
|
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pronounced dead: |
|
|
|
|
|
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Infant’s information: |
|
Last: |
|
|
|
|
|
|
First: |
|
|
|
|
|
|
M: |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Sex: |
|
Male |
|
|
Female |
Date of Birth: |
|
|
|
|
|
|
|
|
Age: |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
Race: |
|
White |
|
|
Black/African Am. |
|
|
Asian/Paciic Islander |
|||||||||||||||||
|
|
|
|
|
|||||||||||||||||||||
|
|
Am. Indian/Alaskan Native |
|
Hispanic/Latino |
|
|
|
Other: |
|
||||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone:
Case #:
1
Sleeping Environment
Infant History
Family Info
Exam |
InsightInvestigator
2
Pathologist
Indicate whether preliminary investigation suggests any of the following:
Yes No
Asphyxia (ex. overlying, wedging, choking, nose/mouth obstruction,
Change in sleep condition (ex. unaccustomed stomach sleep position, location, or sleep surface)
Hyperthermia/Hypothermia (ex. excessive wrapping, blankets, clothing, or hot or cold environments)
Environmental hazards (ex. carbon monoxide, noxious gases, chemicals, drugs, devices)
Unsafe sleep condition (ex. couch/sofa, waterbed, stuffed toys, pillows, soft bedding)
Diet (e.g., solids introduced, etc.)
Recent hospitalization
Previous medical diagnosis
History of acute
History of medical care without diagnosis
Recent fall or other injury
History of religious, cultural, or ethnic remedies
Cause of death due to natural causes other than SIDS (ex. birth defects, complications of preterm birth) Prior sibling deaths
Previous encounters with police or social service agencies
Request for tissue or organ donation
Objection to autopsy
Death due to trauma (injury), poisoning, or intoxication
Suspicious circumstances
Other alerts for pathologist’s attention
Any “Yes” answers above should be explained in detail (description of circumstances):
Pathologist information |
Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Agency: |
|
|
|
Phone: |
|
Fax: |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
Page 8