SURGERY SCHEDULING SHEET &
PHYSICIANS PRE-ADMISSION TESTING ORDERS
PLEASE FAX TO 866-647-0527, ALONG WITH COPY OF INSURANCE CARD
NAME |
|
|
SURGERY DATE |
ARRIVAL TIME |
SURGERY TIME |
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS |
|
|
PROCEDURE & CPT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
**CIRCLE ONE** |
R |
L |
|
|
|
|
|
|
|
PHONE (H) |
|
|
DIAGNOSIS & ICD9 |
|
|
|
|
|
|
|
|
|
|
PHONE (W) |
|
(C) |
|
|
|
|
|
|
|
|
|
|
|
SS# |
|
|
SURGEON |
|
|
|
|
|
|
|
|
|
|
DOB |
|
|
REFERRING PHYSICIAN |
|
|
|
|
|
|
|
|
|
|
ALLERGIES |
|
|
PCP |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ANESTHESIA TYPE |
|
|
|
|
|
|
|
|
|
|
|
|
|
**CIRCLE ONE** |
OP |
|
23HR OBSERVATION |
INPATIENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
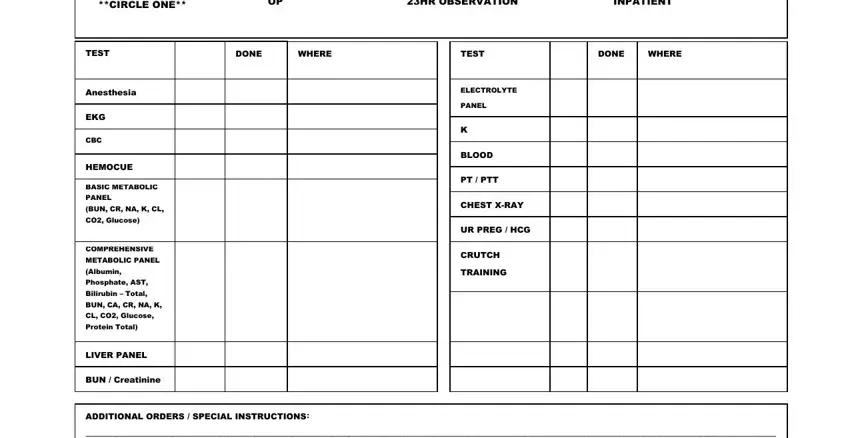
|
TEST |
DONE |
WHERE |
Anesthesia |
|
|
EKG |
|
|
CBC |
|
|
HEMOCUE |
|
|
BASIC METABOLIC |
|
|
PANEL |
|
|
(BUN, CR, NA, K, CL, |
|
|
CO2, Glucose) |
|
|
COMPREHENSIVE METABOLIC PANEL (Albumin, Phosphate, AST, Bilirubin – Total, BUN, CA, CR, NA, K, CL, CO2, Glucose, Protein Total)
LIVER PANEL
BUN / Creatinine
ELECTROLYTE
PANEL
K
BLOOD
PT / PTT
CHEST X-RAY
UR PREG / HCG
CRUTCH
TRAINING
ADDITIONAL ORDERS / SPECIAL INSTRUCTIONS:
_________________________________________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________________________________________
_________________________________________________________________ |
_________________________________________________________________________ |
**PHYSICIAN’S SIGNATURE** |
DATE |
PATIENT NAME:______________________________________________
SURGERY PROCEDURE:________________________________________
SURGEON:__________________________________________________
DATE OF SURGERY:___________________________________________
TIME OF SURGERY:_____________ ARRIVAL TIME:_________________
PATIENT INFORMATION:
Our professional staff is dedicated to providing the highest quality of individualized care to each of our patients. This patient focused approach is intended to promote long term health and well being that results in a high degree of patient satisfaction.
We want to make your upcoming visit as pleasant and comfortable as possible. To make your surgery a successful experience, please read and follow the information on the enclosed sheet.
DAY OF SURGERY:
OArrive promptly at the scheduled time. This will allow adequate time for all necessary pre-surgery procedures.
OPlease bring your insurance identification cards. If special financial arrangements are necessary, please call the Medical Center prior to arrival.
OBe sure to bring any paperwork your doctor gave you, such as test results and/or films, and a list of all medications you are taking.
OWear comfortable, loose fitting clothing.
OUpon arrival, you will change into a gown and slippers which we will provide. You will be asked to remove contact lenses, dentures and any prosthesis.
PREPARING FOR YOUR SURGERY:
Sometime before your surgery date, a staff member from the Medical Center will call you to confirm your surgery time.
They will also ask you questions regarding current and past medical conditions, allergies and medications you are taking. Please don’t hesitate to ask any questions you may have. Be sure to let the staff know of any special needs.
OYou will be instructed as to what time you are to stop eating and drinking prior to your surgery and what medications you should or should not take.
OFor women, if there is any possibility you are pregnant, please notify your doctor and the Medical Center nurse.
OLeave all valuables at home, including watches, rings, jewelry and wallets.
ONotify your surgeon of any changes in your health such as a cold or fever.
OFor your safety, please arrange for an adult to drive you home after surgery. You will not be allowed to drive yourself home.

 MEDICAL CENTER at ELIZABETH PLACE
MEDICAL CENTER at ELIZABETH PLACE
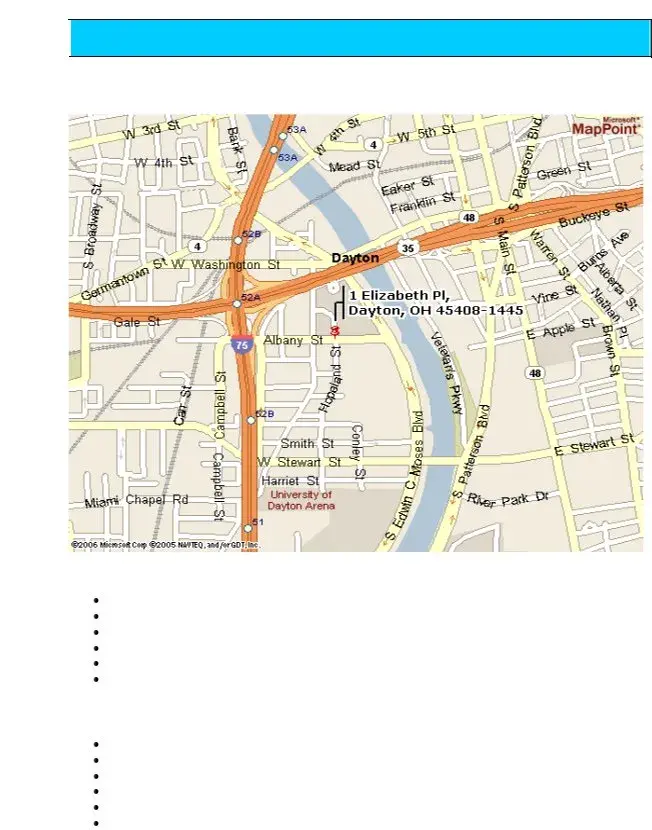
1 Elizabeth Pl, Dayton, OH 45408-1445 |
Telephone: 937-223-MCEP |
DIRECTIONS and MAP
From South of Dayton
Take I-75 NORTH into Dayton
Take the Edwin C. Moses exit (#51)
Turn RIGHT at the end of the exit ramp onto Edwin C. Moses
Follow Edwin C. Moses just over 1 mile
Turn left onto Albany St (before the Dayton Heart Hospital)
Turn right onto Elizabeth Place
From North of Dayton
Take I-75 SOUTH into Dayton
Stay on I-75 (approximately 14 miles south of I-70)
Take the Albany Street exit
Turn LEFT at the end of the exit ramp onto Albany Street
Turn LEFT onto Cincinnati Street (at a 4-way stop)
Turn RIGHT onto Elizabeth Place
Valet Parking available in front of the West Pavilion (no charge). Enter through main entrance; turn right to go to the elevators. Take the elevator to the second floor; the medical center is to the left.