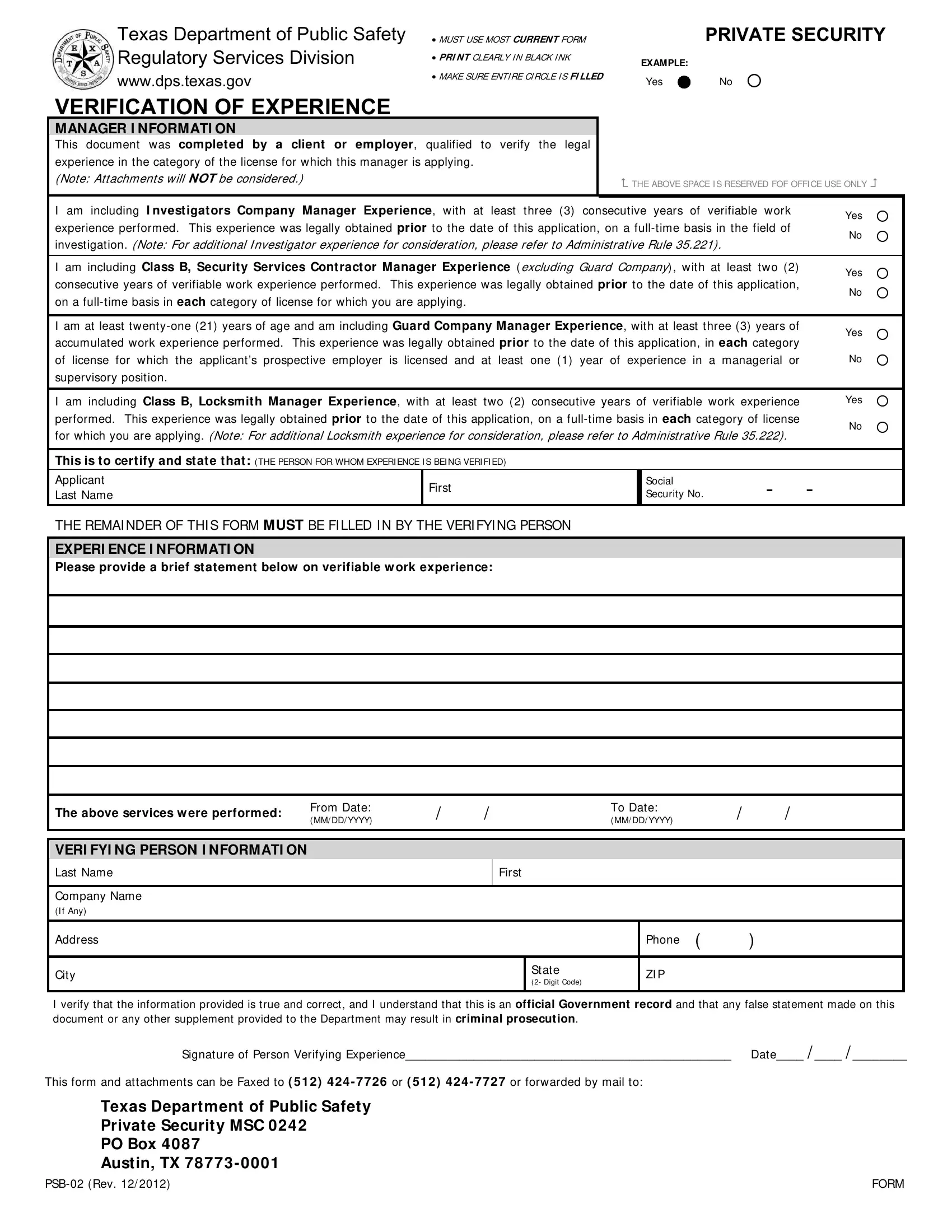
In the heart of Texas, the Verification of Experience form emerges as a crucial document, especially for those navigating the intricacies of the state's legal requirements for security and locksmith fields. Managed by the Texas Department of Public Safety Regulatory Services Division, this form serves as a formal verification tool, mandating a clear, ink-black print to ensure the information is legible. It is imperative for individuals applying for managerial positions in private security or as locksmith managers to meticulously fill out this form, highlighting their verifiable work experience. With sections dedicated to Manager Information and Experience Information, the form acts as a gateway for applicants to prove their qualifications in specific categories of licences — each with its predefined experience prerequisites. For instance, a prospective Investigator Company Manager must document at least three consecutive years of relevant, full-time work experience. Similarly, requirements for other roles vary, like the Guard Company Manager needing three years of accumulated experience. Beyond just listing experience, the form demands certification from a verifying individual, ensuring that all claims made are not only accurate but certified under the risk of criminal prosecution for falsehoods. The delicate process culminates with the option to submit the form via fax or mail, marking the culmination of a crucial step in cementing one's professional standing in Texas' security sector.
| Question | Answer |
|---|---|
| Form Name | Texas Form Verification |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | tx psb forms, texas psb online, texas form psb, texas notary verification form |
Texas Department of Public Safety Regulatory Services Division
www.dps.texas.gov
VERIFICATION OF EXPERIENCE
MUST USE MOST CURRENT FORM |
|
|
PRIVATE SECURITY |
|
|
|
|
PRI NT CLEARLY I N BLACK I NK |
EXAMPLE: |
|
|
|
|
||
MAKE SURE ENTI RE CI RCLE I S FI LLED |
Yes |
|
No |
|
|||
MANAGER I NFORMATI ON
This document was complet ed by a client or employer, qualified to verify the legal experience in the category of the license for which this manager is applying.
(Note: Attachments will NOT be considered.)
THE ABOVE SPACE I S RESERVED FOF OFFI CE USE ONLY
I am including I nvestigators Company Manager Experience, with at least three (3) consecutive years of verifiable work |
Yes |
|
|
experience performed. This experience was legally obtained prior to the date of this application, on a |
|||
No |
|
||
investigation. (Note: For additional I nvestigator experience for consideration, please refer to Administrative Rule 35.221) . |
|||
|
|
||
|
|
|
|
I am including Class B, Security Services Contractor Manager Experience ( excluding Guard Company), with at least two (2) |
Yes |
|
|
consecutive years of verifiable work experience performed. This experience was legally obtained prior to the date of this application, |
|||
No |
|
||
on a |
|||
|
|
||
|
|
|
|
I am at least |
Yes |
|
|
accumulated work experience performed. This experience was legally obtained prior to the date of this application, in each category |
|||
|
|
||
of license for which the applicant’s prospective employer is licensed and at least one (1) year of experience in a managerial or |
No |
|
|
supervisory position. |
|
|
I am including Class B, Locksmith Manager Experience, with at least two (2) consecutive years of verifiable work experience |
Yes |
|
performed. This experience was legally obtained prior to the date of this application, on a |
No |
|
for which you are applying. (Note: For additional Locksmith experience for consideration, please refer to Administrative Rule 35.222) . |
||
|
This is to certify and state that: (THE PERSON FOR WHOM EXPERI ENCE I S BEI NG VERI FI ED)
Applicant |
First |
Social |
- |
- |
|
Last Name |
Security No. |
||||
|
|||||
|
|
|
|
|
THE REMAI NDER OF THI S FORM MUST BE FI LLED I N BY THE VERI FYI NG PERSON
EXPERI ENCE I NFORMATI ON
Please provide a brief statement below on verifiable w ork experience:
The above services w ere performed: |
From Date: |
/ |
/ |
To Date: |
/ |
/ |
(MM/ DD/ YYYY) |
(MM/ DD/ YYYY) |
VERI FYI NG PERSON I NFORMATI ON
Last Name
Company Name
(I f Any)
First
Address
City
|
Phone ( |
) |
|
|
|
State |
ZI P |
|
(2- Digit Code) |
|
|
|
|
|
|
|
|
I verify that the information provided is true and correct, and I understand that this is an official Government record and that any false statement made on this document or any other supplement provided to the Department may result in criminal prosecution.
Signature of Person Verifying Experience________________________________________________ Date____ / ____ / ________
This form and attachments can be Faxed to ( 512) 424 - 7726 or ( 512) 424 - 7727 or forwarded by mail to:
Texas Department of Public Safety
Private Security MSC 0242
PO Box 4087
Austin, TX 78773 - 0001
FORM |