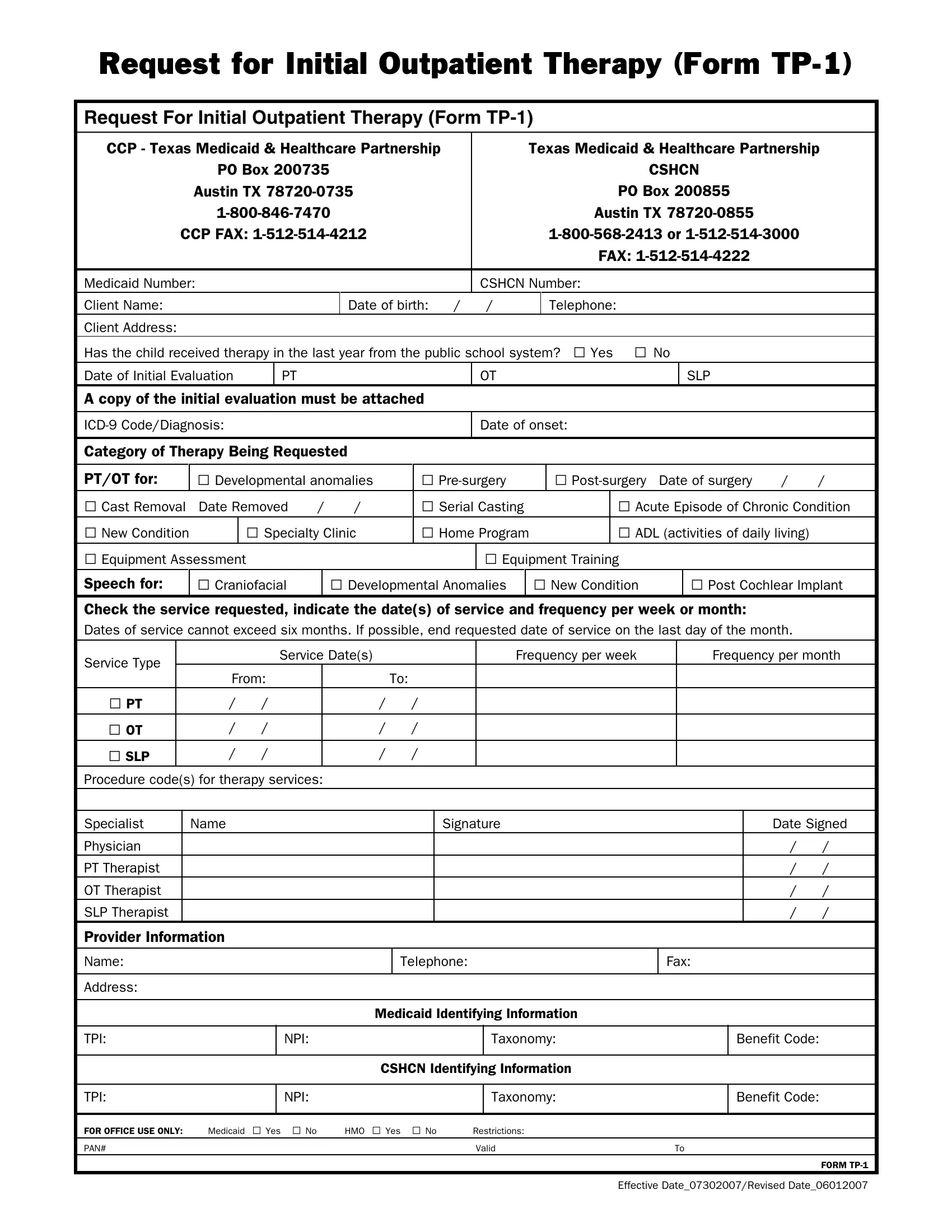
Navigating the healthcare system can often feel like a daunting endeavor, especially when it entails securing essential services for children with special needs. The Request for Initial Outpatient Therapy, commonly known as Form TP-1, serves as a critical bridge for parents and guardians navigating the Texas Medicaid & Healthcare Partnership. This comprehensive form, detailed in its approach, is designed for the initiation of outpatient therapy services across various disciplines – including physical therapy (PT), occupational therapy (OT), and speech-language pathology (SLP). For Texas residents, understanding the nuances of this form is vital. The form not only requests basic information such as the child's Medicaid or CSHCN (Children with Special Health Care Needs) number, name, date of birth, and address, but it also dives deeper into the child's medical history, inquiring about recent therapy received in public schools. Furthermore, it necessitates specifics about the therapy being sought, such as the type of condition (e.g., developmental anomalies, postsurgical requirements, or acute episodes of chronic conditions) and the desired frequency of sessions. With spaces for detailed provider information and necessary approvals, the TP-1 form stands as an organized method to request and document the essential therapy services, paving the way for improved health outcomes for children under its coverage.
| Question | Answer |
|---|---|
| Form Name | Tp 1 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Request for Initial Outpatient Therapy (TP1) tp1 medicaid form |
Request for Initial Outpatient Therapy (Form
Request For Initial Outpatient Therapy (Form
CCP - Texas Medicaid & Healthcare Partnership |
|
Texas Medicaid & Healthcare Partnership |
||||
PO Box 200735 |
|
|
CSHCN |
|||
Austin TX |
|
|
PO Box 200855 |
|||
|
|
|
Austin TX |
|||
CCP FAX: |
|
|
||||
|
|
|
|
|
FAX: |
|
|
|
|
|
|
|
|
Medicaid Number: |
|
|
CSHCN Number: |
|||
Client Name: |
|
Date of birth: / |
/ |
|
Telephone: |
|
Client Address: |
|
|
|
|
|
|
Has the child received therapy in the last year from the public school system? □ Yes □ No |
||||||
Date of Initial Evaluation |
PT |
OT |
|
|
SLP |
|
A copy of the initial evaluation must be attached |
|
|
|
|
||
Date of onset:
Category of Therapy Being Requested
PT/OT for: |
□ Developmental anomalies |
□ |
|
□ |
Date of surgery |
/ |
/ |
||||||||
□ Cast Removal |
Date Removed |
/ |
/ |
□ Serial Casting |
|
|
□ Acute Episode of Chronic Condition |
||||||||
□ New Condition |
|
□ Specialty Clinic |
□ Home Program |
|
|
□ ADL (activities of daily living) |
|
||||||||
□ Equipment Assessment |
|
|
|
|
|
□ Equipment Training |
|
|
|
|
|
||||
Speech for: |
□ Craniofacial |
|
|
□ Developmental Anomalies |
|
□ New Condition |
|
□ Post Cochlear Implant |
|||||||
Check the service requested, indicate the date(s) of service and frequency per week or month:
Dates of service cannot exceed six months. If possible, end requested date of service on the last day of the month.
Service Type |
|
Service Date(s) |
|
|
Frequency per week |
Frequency per month |
|
From: |
|
|
To: |
|
|
||
|
|
|
|
|
|||
□ PT |
/ |
/ |
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
□ OT |
/ |
/ |
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
□ SLP |
/ |
/ |
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
Procedure code(s) for therapy services:
Specialist |
Name |
Signature |
Physician |
|
|
PT Therapist |
|
|
OT Therapist |
|
|
SLP Therapist |
|
|
|
|
|
Date Signed
/ |
/ |
/ |
/ |
/ |
/ |
/ |
/ |
Provider Information
Name: |
Telephone: |
Fax: |
|
|
|
Address:
Medicaid Identifying Information
TPI:
NPI:
Taxonomy:
Benefit Code:
CSHCN Identifying Information
TPI:
NPI:
Taxonomy:
Benefit Code:
FOR OFFICE USE ONLY: |
Medicaid □ Yes □ No |
HMO □ Yes □ No |
Restrictions: |
|
PAN# |
|
|
Valid |
To |
|
|
|
|
FORM |
|
|
|
|
Effective Date_07302007/Revised Date_06012007 |