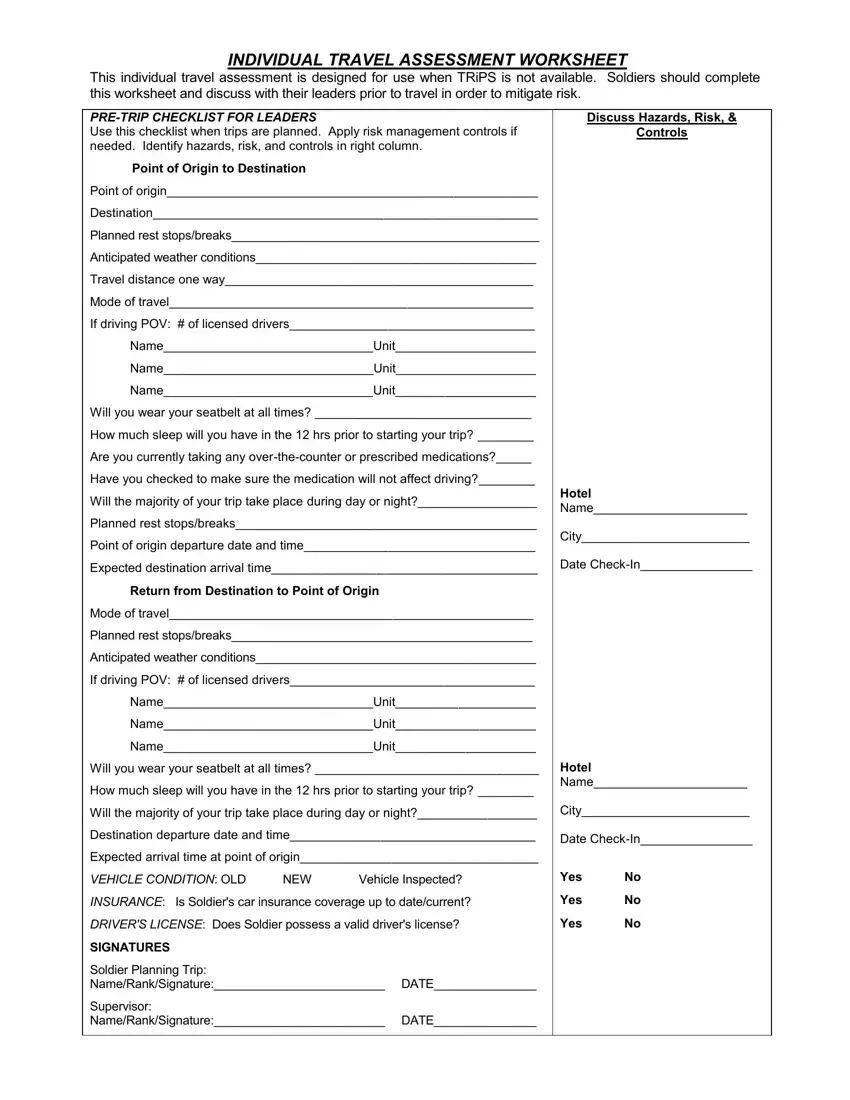
PRE-TRIP CHECKLIST FOR LEADERS
Use this checklist when trips are planned. Apply risk management controls if needed. Identify hazards, risk, and controls in right column.
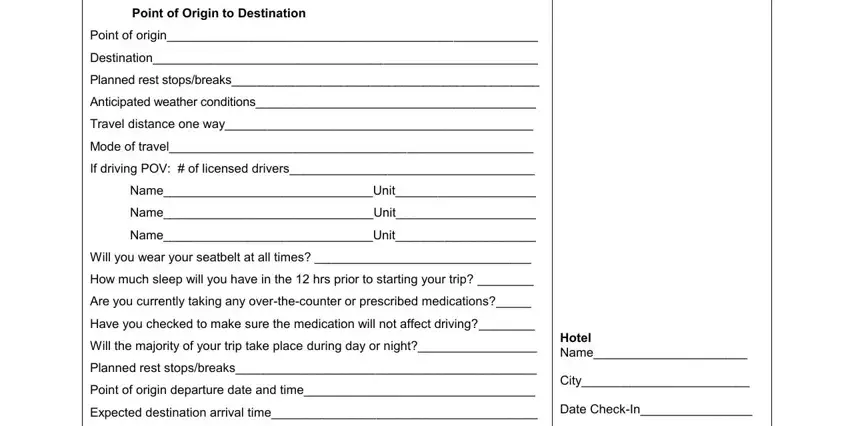
Point of Origin to Destination
Point of origin_____________________________________________________
Destination_______________________________________________________
Planned rest stops/breaks_____________________________________________
Anticipated weather conditions_________________________________________
Travel distance one way____________________________________________
Mode of travel____________________________________________________
If driving POV: # of licensed drivers___________________________________
Name______________________________Unit____________________
Name______________________________Unit____________________
Name______________________________Unit____________________
Will you wear your seatbelt at all times? _______________________________
How much sleep will you have in the 12 hrs prior to starting your trip? ________
Are you currently taking any over-the-counter or prescribed medications?_____
Have you checked to make sure the medication will not affect driving?________
Will the majority of your trip take place during day or night?_________________
Planned rest stops/breaks___________________________________________
Point of origin departure date and time_________________________________
Expected destination arrival time______________________________________
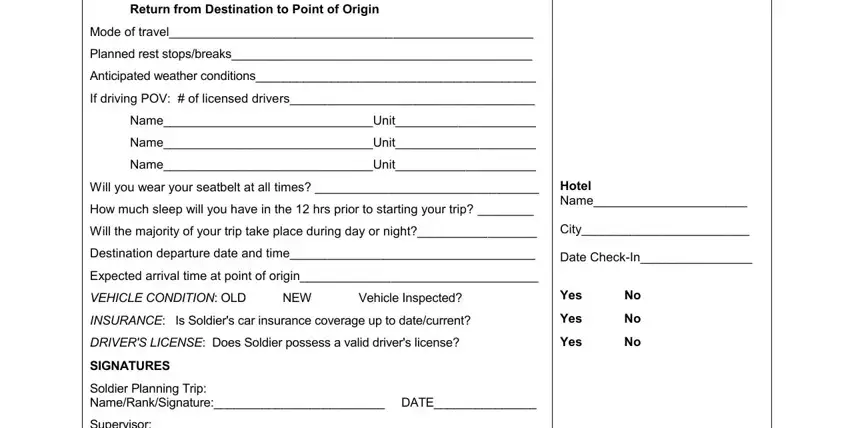
Return from Destination to Point of Origin
Mode of travel____________________________________________________
Planned rest stops/breaks____________________________________________
Anticipated weather conditions_________________________________________
If driving POV: # of licensed drivers___________________________________
Name______________________________Unit____________________
Name______________________________Unit____________________
Name______________________________Unit____________________
Will you wear your seatbelt at all times? ________________________________
How much sleep will you have in the 12 hrs prior to starting your trip? ________
Will the majority of your trip take place during day or night?_________________
Destination departure date and time___________________________________
Expected arrival time at point of origin__________________________________
VEHICLE CONDITION: OLD |
NEW |
Vehicle Inspected? |
INSURANCE: Is Soldier's car insurance coverage up to date/current? |
DRIVER'S LICENSE: Does Soldier possess a valid driver's license? |
SIGNATURES |
|
|
|
Soldier Planning Trip: |
|
|
|
Name/Rank/Signature:_________________________ |
DATE_______________ |
Supervisor: |
|
|
|
Name/Rank/Signature:_________________________ |
DATE_______________ |