

Through the online editor for PDFs by FormsPal, you're able to fill out or change Trsl Form 15 here and now. To maintain our tool on the cutting edge of practicality, we strive to integrate user-driven capabilities and enhancements on a regular basis. We are at all times happy to get suggestions - join us in revolutionizing how we work with PDF files. Here's what you will have to do to get going:
Step 1: Just click the "Get Form Button" at the top of this page to launch our pdf editing tool. Here you'll find everything that is required to work with your file.
Step 2: The editor will allow you to change PDF files in a range of ways. Enhance it by including personalized text, adjust original content, and put in a signature - all manageable within a few minutes!
This PDF form requires specific data to be typed in, hence you should definitely take your time to provide what's expected:
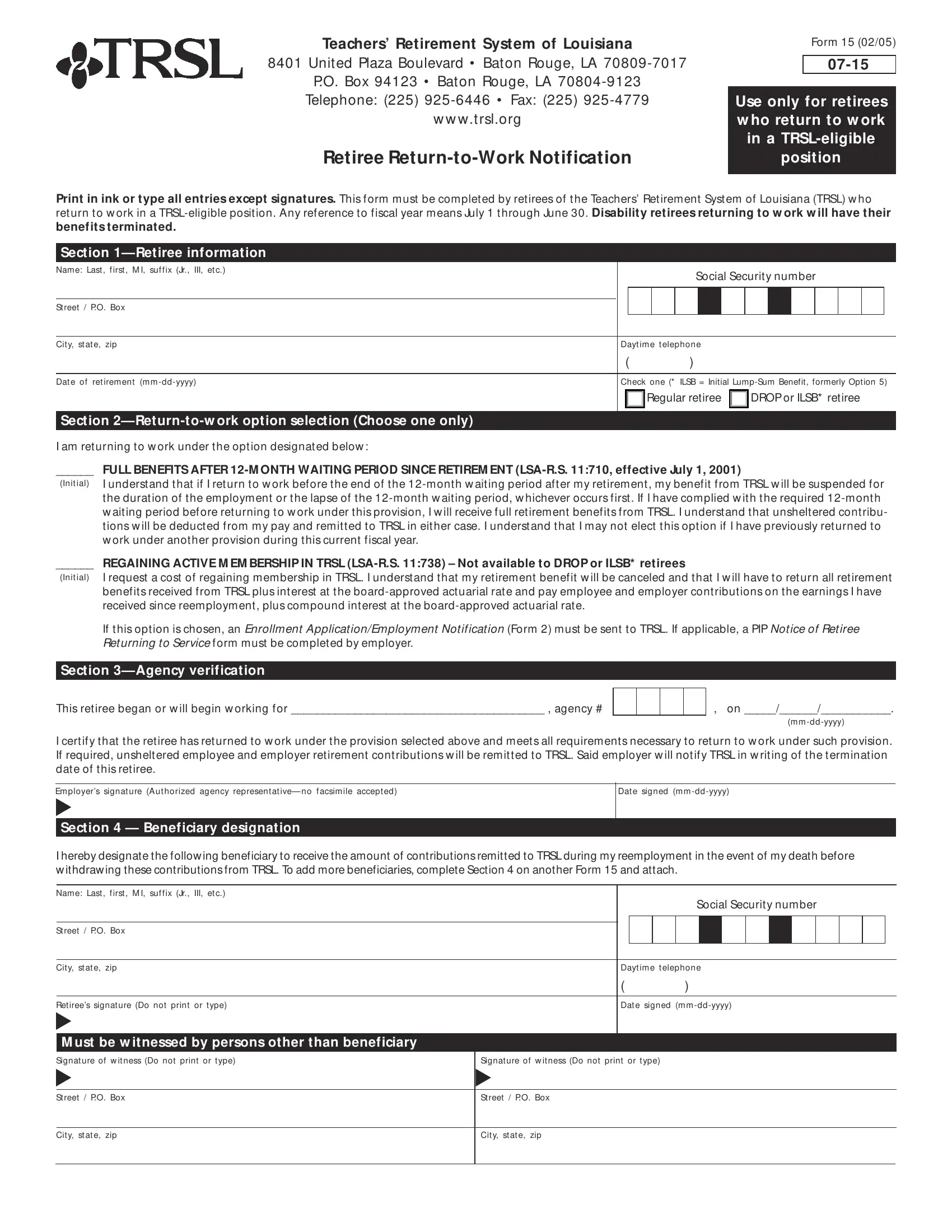
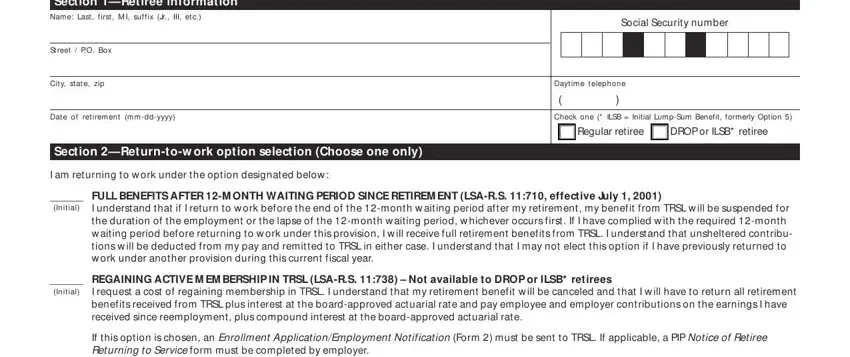
1. To begin with, while filling in the Trsl Form 15, beging with the area that contains the subsequent blank fields:
2. Once your current task is complete, take the next step – fill out all of these fields - Section Agency verification, This retiree began or w ill begin, m m ddyyyy, I certify that the retiree has, Em ployers signat ure Aut horized, Dat e signed m m ddyyyy, Section Beneficiary designation, I hereby designate the follow ing, Name Last f irst M I suf f ix Jr, St reet PO Box, Cit y st at e zip, Ret irees signat ure Do not print, M ust be w itnessed by persons, Social Security number, and Dayt im e t elephone with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
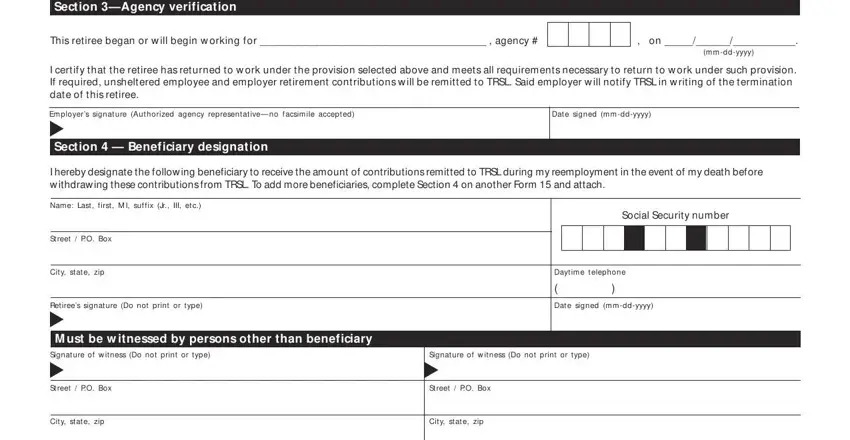
It's easy to make a mistake when filling in the Dat e signed m m ddyyyy, hence you'll want to go through it again before you finalize the form.
Step 3: Go through the information you've inserted in the blanks and then hit the "Done" button. Try a 7-day free trial account with us and acquire immediate access to Trsl Form 15 - available from your FormsPal account. Here at FormsPal.com, we do our utmost to ensure that all of your information is stored protected.