
Should you want to fill out ub 92 revenue codes, it's not necessary to download any kind of software - just make use of our online tool. FormsPal team is dedicated to providing you with the absolute best experience with our editor by regularly presenting new features and enhancements. Our editor is now even more helpful with the newest updates! So now, editing PDF forms is simpler and faster than before. This is what you will want to do to get going:
Step 1: Just click on the "Get Form Button" at the top of this page to get into our form editing tool. This way, you will find everything that is required to fill out your file.
Step 2: The tool lets you customize PDF forms in various ways. Improve it by writing personalized text, correct what is originally in the PDF, and put in a signature - all within a couple of mouse clicks!
It is straightforward to finish the form using this practical guide! Here's what you should do:
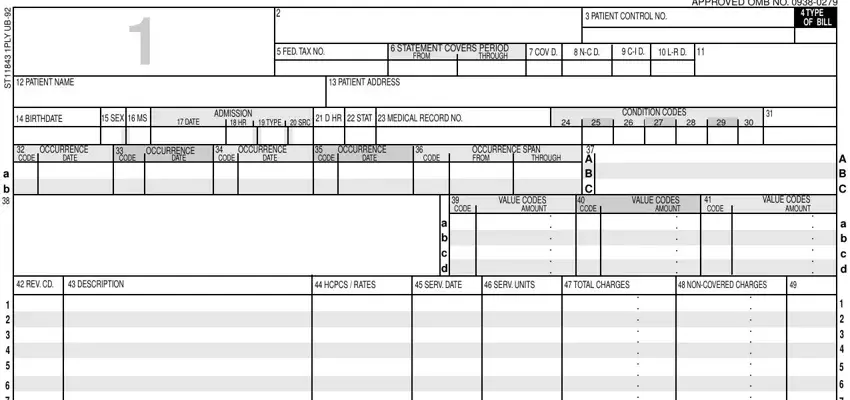
1. Begin completing your ub 92 revenue codes with a group of major blank fields. Collect all of the required information and be sure there's nothing forgotten!
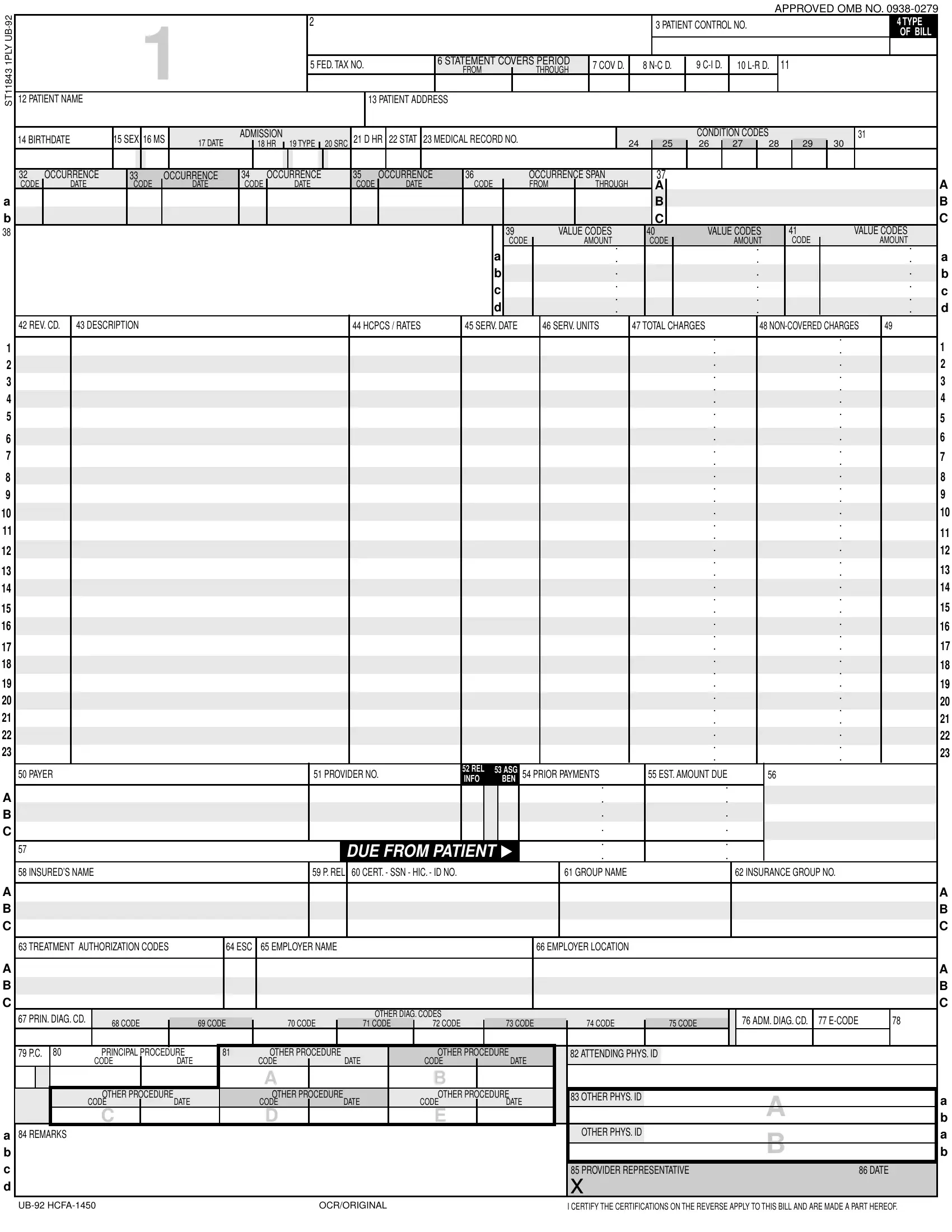
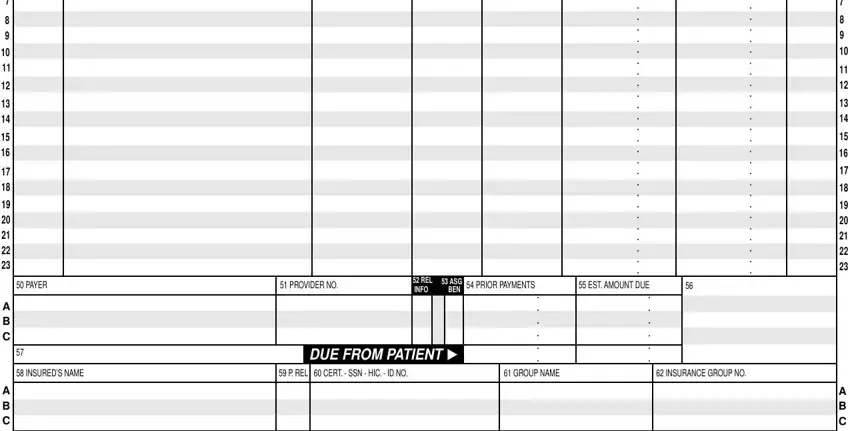
2. After filling in the last part, go on to the subsequent step and enter the essential particulars in all these blank fields - PAYER PROVIDER NO PRIOR, REL INFO, ASG BEN, DUE FROM PATIENT, and INSUREDS NAME P REL CERT SSN.
3. The third stage is generally straightforward - complete all the blanks in TREATMENT AUTHORIZATION CODES, PRIN DIAG CD, CODE CODE CODE CODE CODE, OTHER DIAG CODES, ADM DIAG CD ECODE, PRINCIPAL PROCEDURE OTHER, CODE DATE CODE DATE CODE DATE, A B, OTHER PROCEDURE OTHER PROCEDURE, CODE DATE CODE DATE CODE DATE, C D E, REMARKS, ATTENDING PHYS ID, OTHER PHYS ID, and OTHER PHYS ID in order to complete the current step.
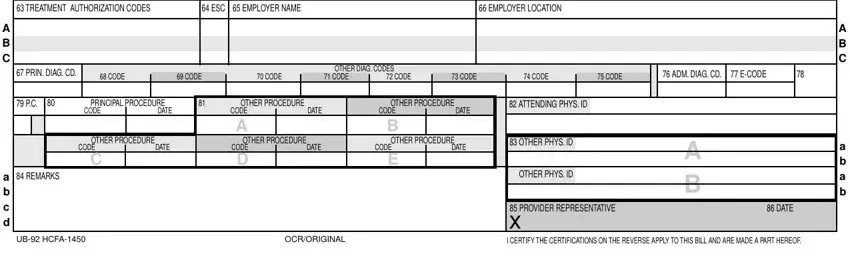
It is easy to get it wrong when filling in the ADM DIAG CD ECODE, therefore you'll want to take a second look prior to deciding to send it in.
Step 3: Spell-check everything you have typed into the blanks and then click on the "Done" button. Get the ub 92 revenue codes once you join for a 7-day free trial. Immediately get access to the form in your FormsPal account, together with any modifications and adjustments conveniently preserved! We don't sell or share any details that you provide whenever working with forms at FormsPal.