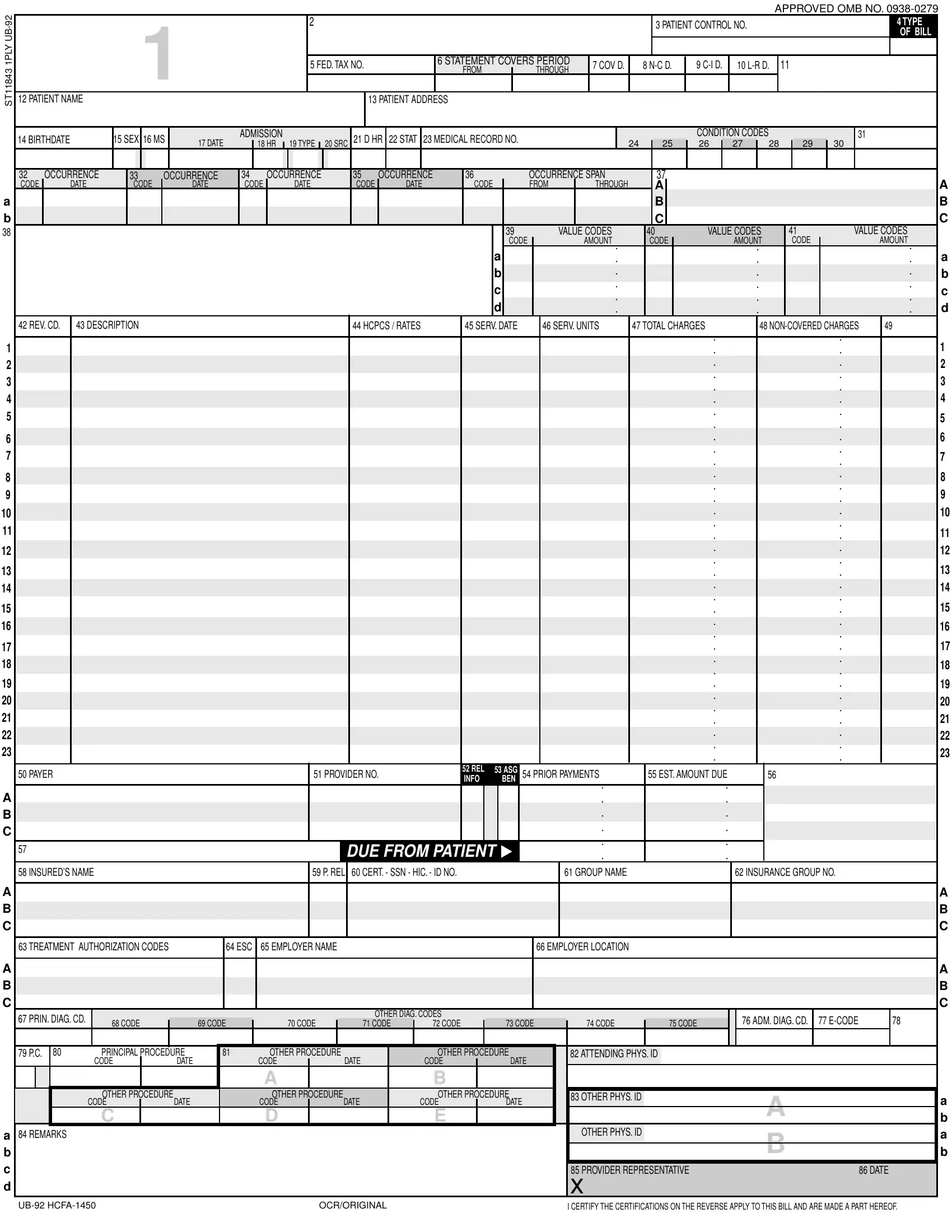
Navigating through medical billing and insurance claims can be complex, and the UB-92 (HCFA-1450) form sits at the heart of this process for many healthcare providers and institutions. This essential document, approved under OMB NO. 0938-0279, serves as a standardized billing form used by hospitals, nursing facilities, and other providers of healthcare services to submit claims to Medicare and Medicaid, as well as private insurers. It encompasses critical patient information, including identification, admission details, and insurance coverage, alongside a detailed rundown of the services provided, coded using the Healthcare Common Procedure Coding System (HCPCS), and the associated charges. The form's structure, divided into sections for patient information, medical condition codes, treatment codes, and financial details, ensures a comprehensive account of the patient's encounter with the healthcare system. By capturing this breadth of data—from the patient's control number and type of bill, through to diagnosis codes, service dates, and charges—the UB-92 form plays a fundamental role in the billing cycle, facilitating the accurate and efficient processing of healthcare claims.
| Question | Answer |
|---|---|
| Form Name | Ub 92 Hcfa 1450 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | DIAG, 1PLY, ub 92, L-R |
ST11843 1PLY
A
B
38
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
A B C
A B C
A B C
A
B
C
D
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
APPROVED OMB NO. |
||||||||||
|
|
|
|
|
|
1 |
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 PATIENT CONTROL NO. |
|
|
|
|
|
|
|
|
4 TYPE |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OF BILL |
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 FED. TAX NO. |
|
|
|
6 STATEMENT COVERS PERIOD |
|
7 COV D. |
|
8 |
9 |
|
10 |
11 |
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FROM |
|
THROUGH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12 PATIENT NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
13 PATIENT ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14 BIRTHDATE |
|
15 SEX |
16 MS |
|
|
ADMISSION |
|
|
|
21 D HR |
22 STAT |
23 MEDICAL RECORD NO. |
|
|
|
|
|
|
|
|
|
CONDITION CODES |
|
|
|
|
|
|
31 |
|
|
|
|
|||||||||||||||
|
|
|
17 DATE |
|
18 HR |
19 TYPE |
20 SRC |
|
|
|
|
24 |
|
25 |
|
26 |
27 |
|
28 |
|
|
29 |
|
30 |
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
37 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
32 |
OCCURRENCE |
|
33 |
|
OCCURRENCE |
34 |
|
OCCURRENCE |
35 |
|
OCCURRENCE |
|
36 |
|
|
|
OCCURRENCE SPAN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
CODE |
|
DATE |
|
CODE |
|
DATE |
CODE |
|
DATE |
CODE |
|
DATE |
|
CODE |
|
FROM |
|
THROUGH |
|
|
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
39 |
VALUE CODES |
|
40 |
|
|
VALUE CODES |
|
|
41 |
|
|
VALUE CODES |
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
CODE |
|
AMOUNT |
|
CODE |
|
|
|
AMOUNT |
|
|
|
CODE |
|
|
|
AMOUNT |
|
A |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
42 REV. CD. |
43 DESCRIPTION |
|
|
|
|
|
|
|
|
|
|
44 HCPCS / RATES |
|
45 SERV. DATE |
46 SERV. UNITS |
47 TOTAL CHARGES |
|
|
48 |
49 |
|
|
||||||||||||||||||||||||||
1 2 3 4 5
6
7
8 9 10
11
12
13
14
15
16
17
18
19 20 21 22 23
|
50 PAYER |
51 PROVIDER NO. |
52 REL |
53 ASG |
54 PRIOR PAYMENTS |
55 EST. AMOUNT DUE |
56 |
|
|||
|
INFO |
|
BEN |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
57 |
|
|
|
|
|
|
|
|
|
|
|
|
DUE FROM PATIENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
58 INSURED’S NAME |
|
|
|
|
59 P. REL |
60 CERT. - SSN - HIC. - ID NO. |
|
|
|
|
61 GROUP NAME |
|
62 INSURANCE GROUP NO. |
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
63 TREATMENT AUTHORIZATION CODES |
|
|
64 ESC |
65 EMPLOYER NAME |
|
|
|
|
|
|
|
66 EMPLOYER LOCATION |
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
|
67 PRIN. DIAG. CD. |
|
|
|
|
|
|
|
|
|
|
OTHER DIAG. CODES |
|
|
|
|
|
|
|
|
76 ADM. DIAG. CD. |
77 |
|
78 |
|
|
||||||
|
|
68 CODE |
|
69 CODE |
70 CODE |
|
71 CODE |
72 CODE |
|
73 CODE |
|
|
|
74 CODE |
|
75 CODE |
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
80 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
79 P.C. |
|
PRINCIPAL PROCEDURE |
|
81 |
OTHER PROCEDURE |
|
|
OTHER PROCEDURE |
|
|
|
82 ATTENDING PHYS. ID |
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
CODE |
|
DATE |
|
|
CODE |
|
|
DATE |
|
CODE |
|
|
DATE |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
A |
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER PROCEDURE |
|
|
|
OTHER PROCEDURE |
|
|
OTHER PROCEDURE |
|
|
|
83 OTHER PHYS. ID |
|
|
A |
|
|
|
A |
|||||||||
|
|
|
|
CODE |
|
|
DATE |
|
|
CODE |
|
|
DATE |
|
CODE |
|
|
DATE |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
C |
|
|
|
|
|
D |
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER PHYS. ID |
|
|
|
|
|
|
|
|
|
|
84 REMARKS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
|
|
|
A |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
85 PROVIDER REPRESENTATIVE |
|
|
86 DATE |
|||||
X
OCR/ORIGINAL |
I CERTIFY THE CERTIFICATIONS ON THE REVERSE APPLY TO THIS BILL AND ARE MADE A PART HEREOF. |