This PDF editor makes it simple to complete the ubh claim form document. It will be easy to build the file in short order by using these simple steps.
Step 1: Pick the button "Get Form Here".
Step 2: So, you can alter the ubh claim form. Our multifunctional toolbar makes it easy to add, get rid of, adapt, highlight, as well as do other commands to the content material and fields inside the file.
The PDF template you wish to prepare will include the next areas:
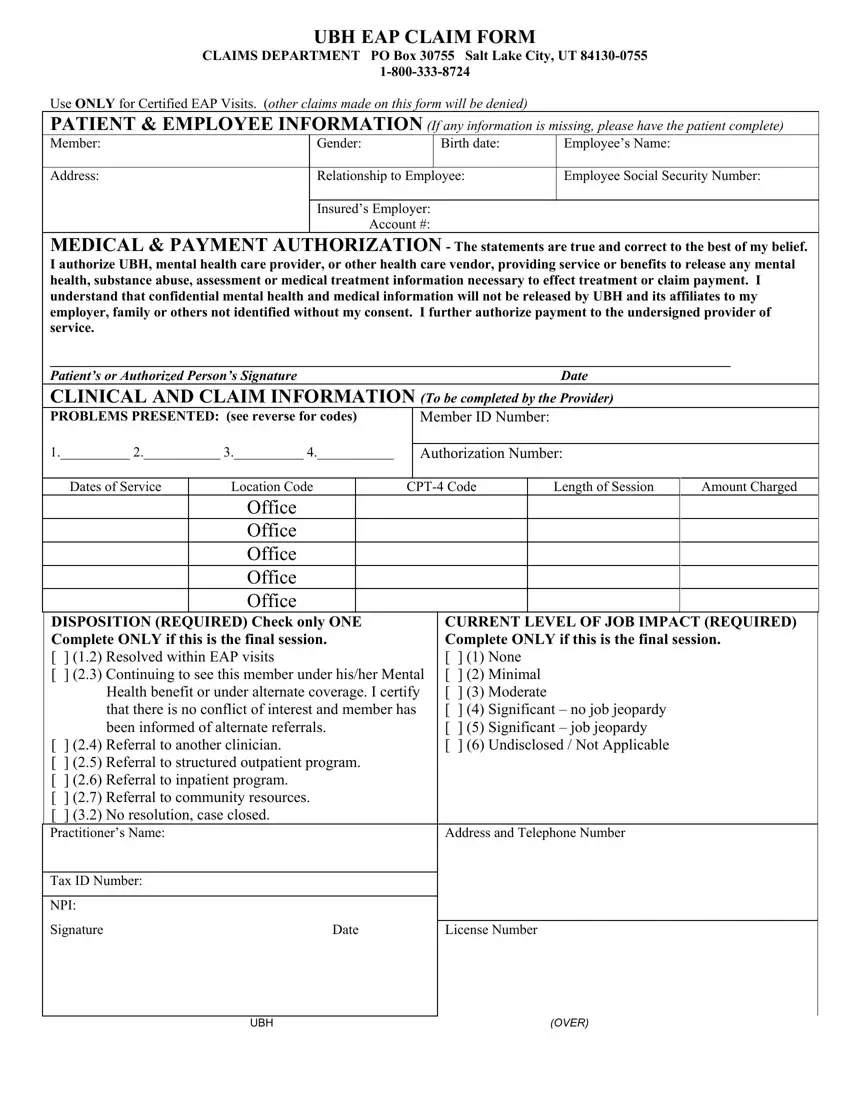
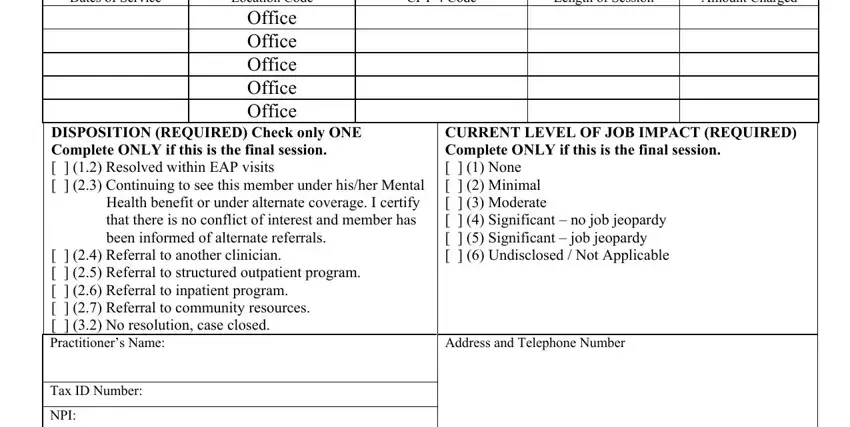
Provide the requested information in the area CPT Code, Length of Session, Amount Charged, Dates of Service, Location Code Office Office Office, DISPOSITION REQUIRED Check only, Referral to another clinician, CURRENT LEVEL OF JOB IMPACT, Address and Telephone Number, Tax ID Number, and NPI.
Put in writing all data you need within the section Signature Date, License Number, UBH, and OVER.
Step 3: Select the button "Done". Your PDF form is available to be exported. You can obtain it to your laptop or send it by email.
Step 4: It is more convenient to save copies of the document. You can rest easy that we won't share or read your particulars.
