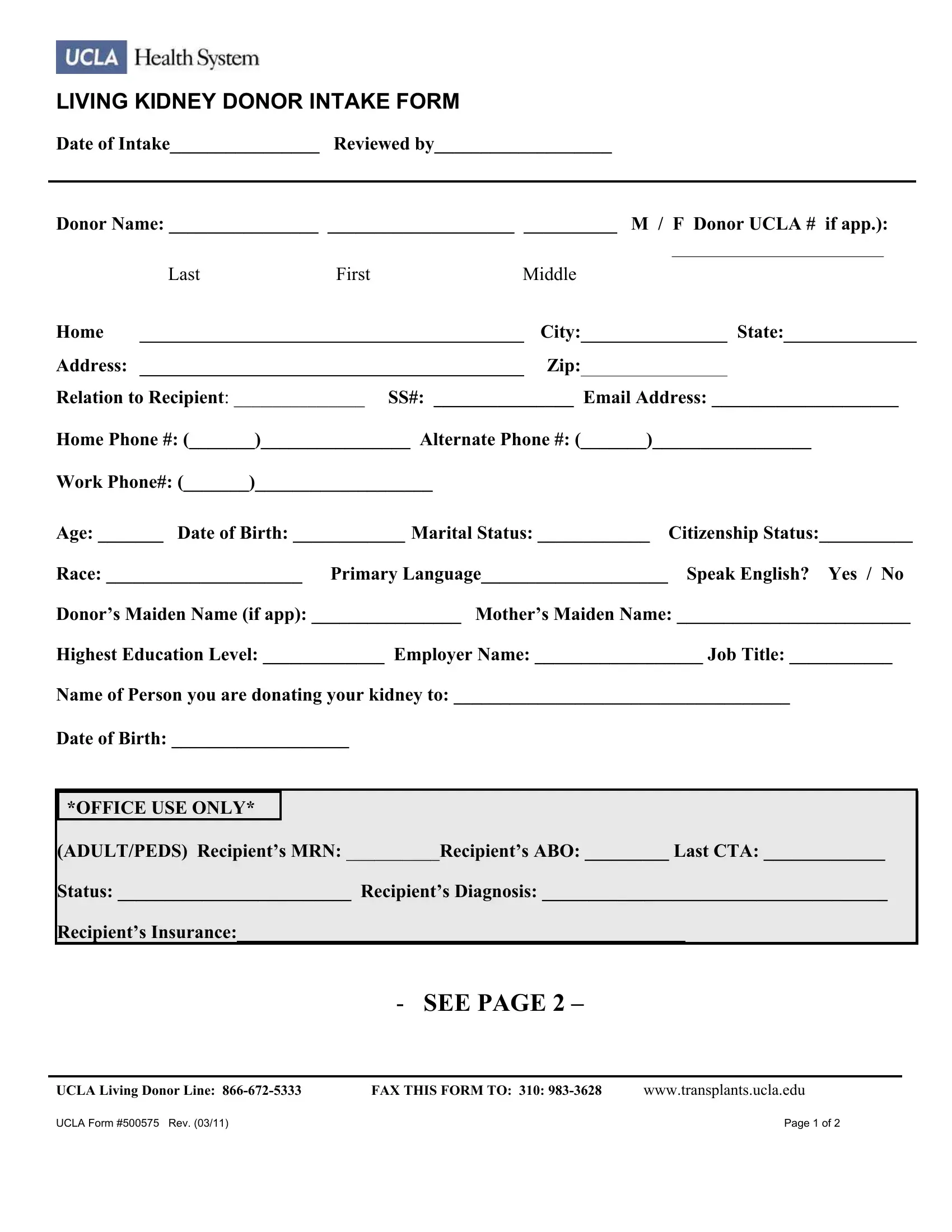
Embarking on the journey of living kidney donation is a commendable and intricate process that involves numerous steps to ensure both donor and recipient’s safety and compatibility. At the heart of this process is the UCLA 500575 form, a comprehensive document designed to meticulously gather the potential donor's detailed information. This Living Kidney Donor Intake Form, updated last in March 2011, serves as the initial screening tool for those willing to offer the gift of life. It records essential data such as the donor's personal information, medical history, relation to the recipient, and other health-related questions to assess eligibility. It even goes as far as to inquire about the donor’s highest level of education, employment details, and support systems post-surgery, reflecting UCLA’s holistic approach to donor well-being. Furthermore, the form delves into detailed medical inquiries covering medications, allergies, family medical history, and any previous health concerns, ensuring a thorough medical evaluation. Notably, the form addresses essential logistics and support mechanisms, highlighting the importance of considering the donor's life after the donation. As an invaluable tool in the pre-transplant assessment phase, this form embodies the comprehensive and careful consideration necessary to proceed with living kidney donations, marking the beginning of a life-changing journey for both donor and recipient.
| Question | Answer |
|---|---|
| Form Name | Ucla Form 500575 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | intake form ucla pdf, ucla kidney donor intake form, intake form ucla, donor intake form |
LIVING KIDNEY DONOR INTAKE FORM
Date of Intake________________ Reviewed by___________________
Donor Name: ________________ ____________________ __________ M / F Donor UCLA # if app.):
|
|
|
|
|
___________________________ |
||
|
Last |
First |
Middle |
|
|
|
|
Home |
|
|
City: |
|
State: |
||
|
|
|
|
|
|
|
|
Address: |
|
|
Zip: |
|
|
|
|
|
|
|
|
|
|
|
|
Relation to Recipient: ______________ SS#: _______________ Email Address: ____________________
Home Phone #: (_______)________________ Alternate Phone #: (_______)_________________
Work Phone#: (_______)___________________
Age: _______ Date of Birth: ____________ Marital Status: ____________ |
Citizenship Status:__________ |
Race: _____________________ Primary Language____________________ |
Speak English? Yes / No |
Donor’s Maiden Name (if app): ________________ Mother’s Maiden Name: _________________________
Highest Education Level: _____________ Employer Name: __________________ Job Title: ___________
Name of Person you are donating your kidney to: ____________________________________
Date of Birth: ___________________
*OFFICE USE ONLY*
(ADULT/PEDS) Recipient’s MRN: __________Recipient’s ABO: _________ Last CTA: _____________
Status: _________________________ Recipient’s Diagnosis: _____________________________________
Recipient’s Insurance:________________________________________________
- SEE PAGE 2 –
UCLA Living Donor Line: |
FAX THIS FORM TO: 310: |
www.transplants.ucla.edu |
UCLA Form #500575 Rev. (03/11) |
|
Page 1 of 2 |

LIVING KIDNEY DONOR INTAKE FORM
Donor’s ABO: __________ Ht: __________ Wt: __________
Medications (prescription and
Blood Sugar Problems (yourself or family): __________________________ During pregnancy? ____________
High Blood Pressure (yourself or family): ___________________________ During pregnancy? ____________
Heart Problems (yourself or family): ____________________________________________________________
Any history of melanoma?: __________ If yes, how long ago were you diagnosed?: _____________________
Kidney Stones or Kidney Problems (yourself or family): ____________________ Cancer: ________________
Urine or Kidney Infections: ___________________________ Liver Problems or Hepatitis:________________
Alcohol / Tobacco/Drug Use: ________________________ Mental Health Problems: ____________________
Hospitalizations/Surgeries/Other Health Problems: ________________________________________________
Any bleeding problems? _____________________________________________________________________
Have you been
Have you ever been incarcerated, and if so how long ago? __________________________________________
When was your latest: Pap Smear (Females only) ___________ Mammogram (Females > 40) ______________
Colonoscopy ( > 60) _______________
Have you discussed your intention to donate with your family/significant other? _________________________
Do you have health insurance? _______Who will take care of you after the surgery? _____________________
Signature of Donor _________________________________________________ Date ________________
Signature of Person Filling Out
Report (if other than donor) |
|
Print Name |
Date ______________ |
UCLA Living Donor Line: |
FAX THIS FORM TO: 310: |
www.transplants.ucla.edu |
UCLA Form #500575 Rev. (03/11) |
|
Page 2 of 2 |