
Whenever you want to fill out you authorization release blank, you don't need to install any kind of programs - simply try using our PDF editor. To retain our tool on the forefront of practicality, we aim to implement user-driven features and improvements regularly. We're at all times thankful for any suggestions - join us in remolding how you work with PDF files. In case you are looking to start, this is what you will need to do:
Step 1: Hit the "Get Form" button at the top of this webpage to access our tool.
Step 2: This tool will allow you to customize PDF forms in various ways. Change it with personalized text, adjust what is already in the PDF, and put in a signature - all close at hand!
Completing this document needs thoroughness. Ensure that all required areas are filled in properly.
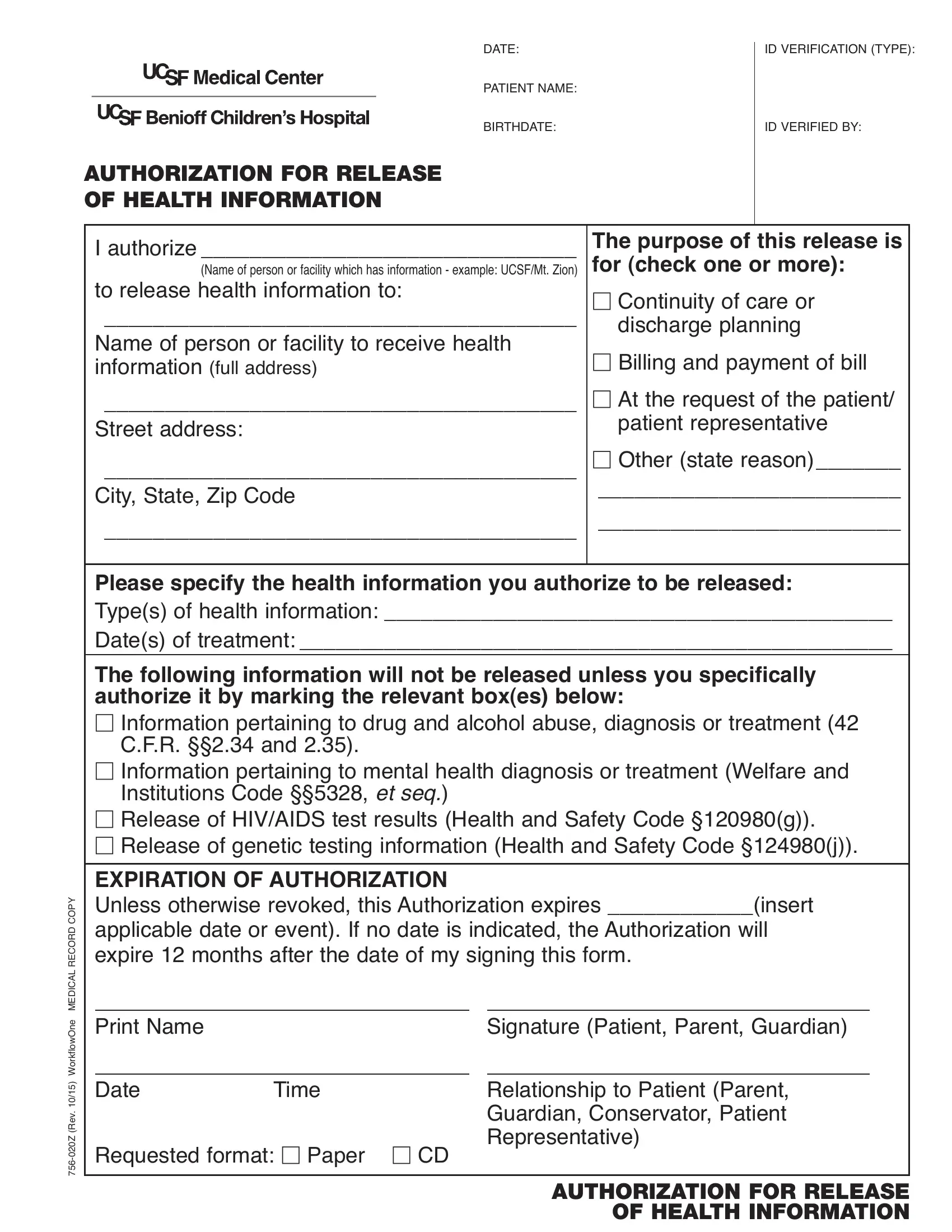
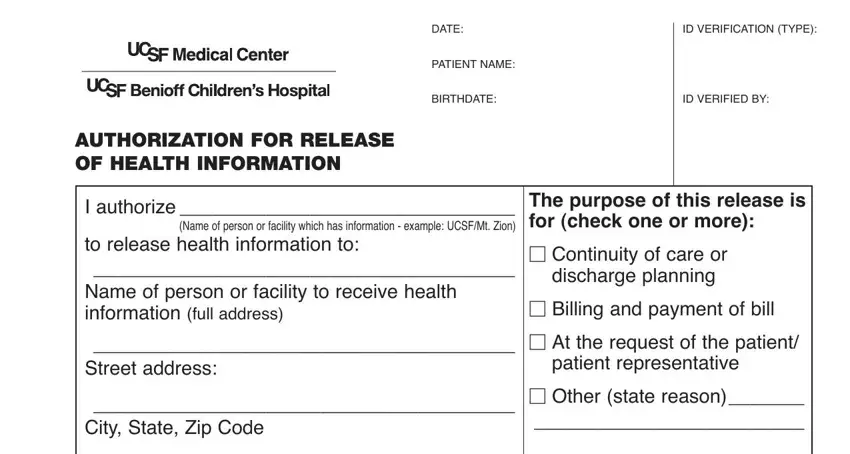
1. It is important to fill out the you authorization release blank properly, thus take care when filling in the segments including all of these blank fields:
2. The third part is usually to fill out all of the following blanks: Please specify the health, The following information will not, CFR and, Information pertaining to mental, Institutions Code et seq, Release of HIVAIDS test results, EXPIRATION OF AUTHORIZATION Unless, Y P O C D R O C E R L A C D E M, e n O w o l f k r o W, v e R, Print Name, Signature Patient Parent Guardian, Date, Time, and Relationship to Patient Parent.
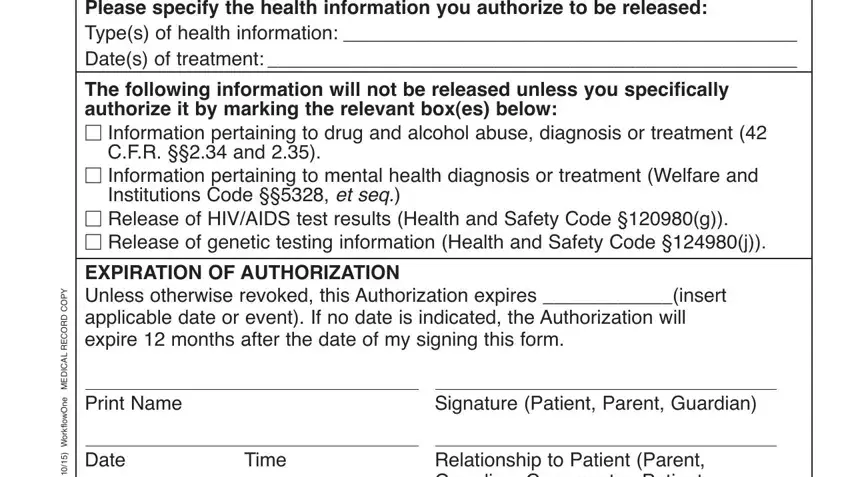
Always be very careful when filling in Institutions Code et seq and Relationship to Patient Parent, because this is where most users make errors.
3. This next portion is about v e R, Requested format Paper CD, Relationship to Patient Parent, and AUTHORIZATION FOR RELEASE OF - fill in each of these fields.

Step 3: When you have reread the details in the fields, click on "Done" to finalize your FormsPal process. Go for a 7-day free trial subscription with us and acquire instant access to you authorization release blank - download, email, or change in your FormsPal account. Here at FormsPal.com, we do everything we can to make certain that all your information is kept protected.