Are you looking for information about the 4M form? This document is essential for any construction project, and it's important to understand what it is and why it should be filled out correctly. In this blog post, we will discuss all aspects of the 4M Form and how it affects your business or construction project. We'll explain exactly what this form entails, why you need to complete the form accurately, provide step-by-step instructions on filing out the 4M form properly and more. Keep reading if you'd like to get a better understanding of when and how to utilize this powerful tool in order to ensure compliance with industry standard regulations!
| Question | Answer |
|---|---|
| Form Name | Ue 4M Form |
| Form Length | 8 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min |
| Other names | new ue nysif online, new york application worker, application worker insurance, state 4m nysif online |
N E W Y O R K S T A T E I N S U R A N C E F U N D
Workers' Compensation and Disability Benefits Specialist since 1914
Document Control Center, 1 Watervliet Ave. Extension, Albany, NY 12206
FOR OFFICE USE ONLY
ATN: _________________
iCMS #: _________________
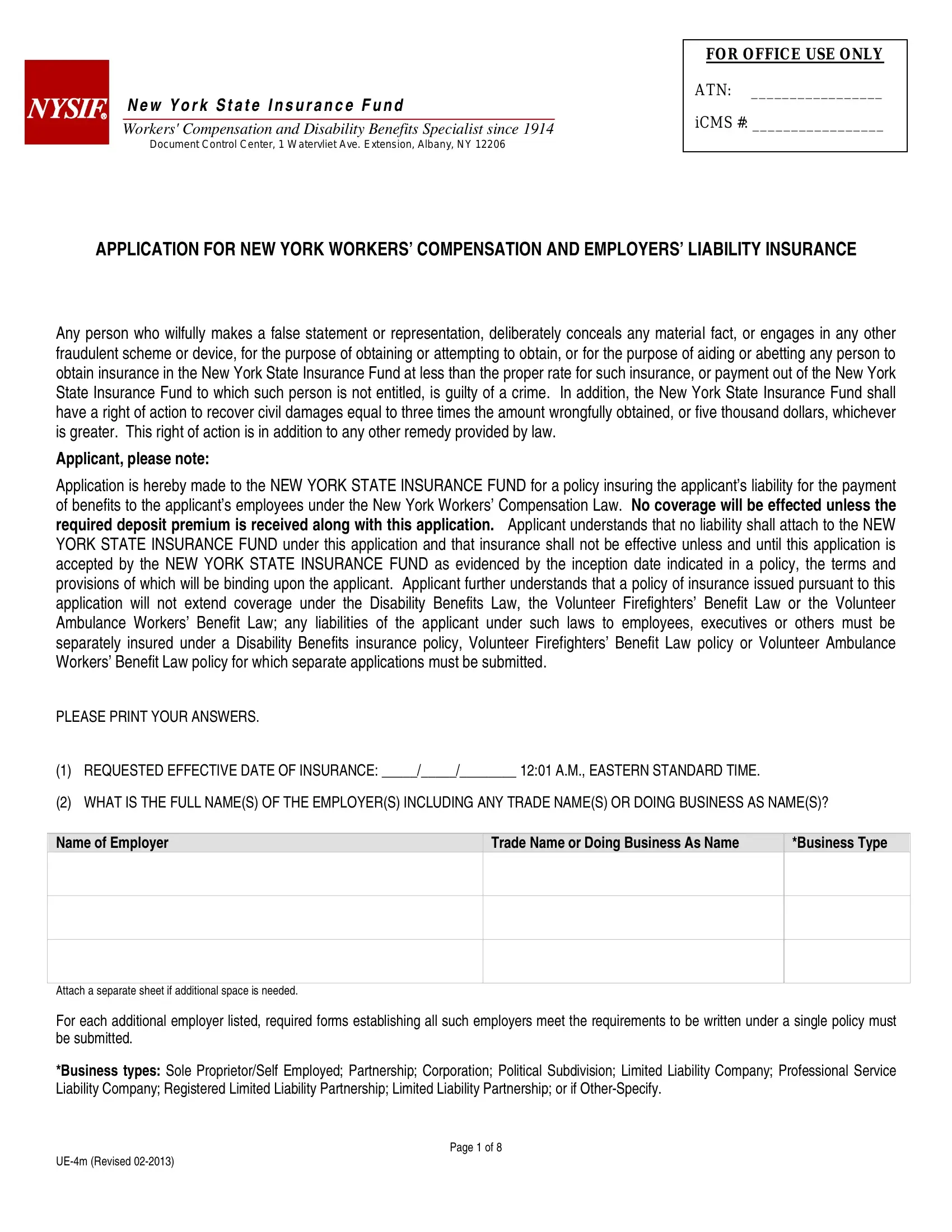
APPLICATION FOR NEW YORK WORKERS’ COMPENSATION AND EMPLOYERS’ LIABILITY INSURANCE
Any person who wilfully makes a false statement or representation, deliberately conceals any material fact, or engages in any other fraudulent scheme or device, for the purpose of obtaining or attempting to obtain, or for the purpose of aiding or abetting any person to obtain insurance in the New York State Insurance Fund at less than the proper rate for such insurance, or payment out of the New York State Insurance Fund to which such person is not entitled, is guilty of a crime. In addition, the New York State Insurance Fund shall have a right of action to recover civil damages equal to three times the amount wrongfully obtained, or five thousand dollars, whichever is greater. This right of action is in addition to any other remedy provided by law.
Applicant, please note:
Application is hereby made to the NEW YORK STATE INSURANCE FUND for a policy insuring the applicant’s liability for the payment of benefits to the applicant’s employees under the New York Workers’ Compensation Law. No coverage will be effected unless the required deposit premium is received along with this application. Applicant understands that no liability shall attach to the NEW YORK STATE INSURANCE FUND under this application and that insurance shall not be effective unless and until this application is accepted by the NEW YORK STATE INSURANCE FUND as evidenced by the inception date indicated in a policy, the terms and provisions of which will be binding upon the applicant. Applicant further understands that a policy of insurance issued pursuant to this application will not extend coverage under the Disability Benefits Law, the Volunteer Firefighters’ Benefit Law or the Volunteer Ambulance Workers’ Benefit Law; any liabilities of the applicant under such laws to employees, executives or others must be separately insured under a Disability Benefits insurance policy, Volunteer Firefighters’ Benefit Law policy or Volunteer Ambulance Workers’ Benefit Law policy for which separate applications must be submitted.
PLEASE PRINT YOUR ANSWERS.
(1)REQUESTED EFFECTIVE DATE OF INSURANCE: _____/_____/________ 12:01 A.M., EASTERN STANDARD TIME.
(2)WHAT IS THE FULL NAME(S) OF THE EMPLOYER(S) INCLUDING ANY TRADE NAME(S) OR DOING BUSINESS AS NAME(S)?
Name of Employer
Trade Name or Doing Business As Name
*Business Type
Attach a separate sheet if additional space is needed.
For each additional employer listed, required forms establishing all such employers meet the requirements to be written under a single policy must be submitted.
*Business types: Sole Proprietor/Self Employed; Partnership; Corporation; Political Subdivision; Limited Liability Company; Professional Service Liability Company; Registered Limited Liability Partnership; Limited Liability Partnership; or if
Page 1 of 8
(3)PLEASE PROVIDE THE MAIN NEW YORK STATE WORK LOCATION OF THE EMPLOYER:
(P.O. BOX IS NOT ACCEPTABLE AS A WORK LOCATION)
For the purpose of serving notice of cancellation in accordance with section 54(5) of the New York Workers’ Compensation Law, the insured(s) agree(s) that service of notice upon the person or entity designated at the address specified is service of notice upon all insureds insured under one insurance policy. All bills, correspondence and other mailed material also will be sent to that person or entity at that address. If an employer identifies a mailing address that is different from the work location address, NYSIF will deem the mailing address the “last known place of business” for cancellation notice purposes.
Address:
City:
Telephone:
Fax:
State:
NY
Zip Code:
-
NEW YORK STATE COUNTY FOR THE EMPLOYER’S MAIN WORK LOCATION:
IS THE WORK LOCATION SHOWN ALSO THE EMPLOYER’S MAILING ADDRESS?
IF NO, PLEASE PROVIDE THE MAILING ADDRESS:
YES
NO
Address:
City:
State:
Zip Code:
-
(4) DO YOU HAVE A REPRESENTATIVE?
YES
NO
(4a) IF YES, PLEASE ENTER INFORMATION ON YOUR REPRESENTATIVE:
Name:
Address:
City: |
|
|
|
State: |
|
|
|
|
|
Telephone: |
|
Fax: |
|
|
|
|
|||
|
|
|
|
|
(5)HOW LONG HAS YOUR COMPANY BEEN IN BUSINESS?
(6)HAVE YOU EVER BEEN INSURED FOR WORKERS’ COMPENSATION?
Requested NYSIF Group No.:
|
|
Zip Code: |
- |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
YEARS |
|
MONTHS |
YES |
NO |
|
(6a) IF YES, PLEASE PROVIDE INFORMATION ON YOUR WORKERS’ COMPENSATION EXPERIENCE FOR THE PAST 5 YEARS:
Year Insurer
Policy #
Annual Premium |
# of Claims |
Total Incurred Claims Cost |
|
|
|
Amount Paid
(7)IF KNOWN, PLEASE ENTER YOUR RATING BOARD FILE NUMBER, LATEST EXPERIENCE MODIFICATION FACTOR AND THE EFFECTIVE RATING DATE:
Rating Board File Number: |
|
Experience Modification Factor: |
|
Effective Rating Date: |
|
|
|
|
|
New York State Insurance Fund Workers’ Compensation and Employers’ Liability Application
Page 2 of 8
/ /
(8)HAVE YOU BEEN DECLINED FOR COVERAGE DURING THE LAST 12 MONTHS?
(8a) IF YES, PLEASE COMPLETE:
YES
NO
Name of Insurance Company
Reason Coverage was Declined
Attach a separate sheet if additional space is needed.
(9) HAVE YOU EVER BEEN INSURED IN THE NEW YORK STATE INSURANCE FUND?
YES
NO
(You must answer “YES” if you or any person who directly or indirectly owns or controls or is the president, vice president, secretary or treasurer of an employer identified in Question (2) either directly or indirectly owns or controls or is president, vice president, secretary or treasurer of an employer that has had a workers’ compensation policy with the State Insurance Fund that was cancelled, or directly or indirectly owned or controlled or was president, vice president, secretary or treasurer of an employer at the time that employer’s workers’ compensation insurance policy with the State Insurance Fund was cancelled. The Workers’ Compensation Law prohibits any person from contracting for a subsequent policy with the State Insurance Fund while the billed premium on such a cancelled policy remains uncollected.)
(9a) IF YES, PLEASE COMPLETE:
Previous State Fund Policy Number |
Period of Coverage |
|
|
|
|
|
|
From: |
/ |
/ |
To: |
/ |
/ |
|
|
|
|
|
|
|
|
From: |
/ |
/ |
To: |
/ |
/ |
|
|
|
|
|
|
|
Attach a separate sheet if additional space is needed. |
|
|
|
|
|
|
(10) PLEASE DESCRIBE YOUR BUSINESS OPERATIONS INCLUDING THE PRODUCTS OR SERVICES SOLD:
If you are a manufacturer, include the raw materials, processes, products, and equipment used or produced. If you are a contractor or engage in construction then describe the type of work performed including the work performed by
Business Description |
(Attach a separate sheet if additional space is needed.) |
|
|
(11) PLEASE LIST YOUR ESTIMATED ANNUAL PAYROLL BY TYPE OF WORK OR DUTIES FOR ALL YOUR EMPLOYEES:
If you are a corporation with one or two executive officers who collectively own 100% of the corporation’s stock, you have the option to exclude the officers from coverage.
DO YOU WISH TO EXCLUDE THE OFFICER(S)? If yes, required forms must be submitted.
YES
NO
If you are a partnership, LLP, PLLP, LLC, PLLC or Sole Proprietorship you can elect to bring partners, members or
DO YOU WISH TO INCLUDE PARTNERS, MEMBERS OR |
YES |
NO |
If yes, include remuneration for person(s) you wish to bring under coverage on the next page and required forms must be submitted.
New York State Insurance Fund Workers’ Compensation and Employers’ Liability Application
Page 3 of 8
QUESTION (11) CONTINUED
Description |
Duties |
# of |
Annual Payroll |
|
|
Employees |
|
CLERICAL OFFICE EMPLOYEES |
|
|
|
SALESPERSONS / COLLECTORS / MESSENGERS
EXECUTIVE OFFICERS / PARTNERS / MEMBERS /
Attach a separate sheet if additional space is needed.
(12)IF YOU ARE A CORPORATION, IN WHAT STATE ARE YOU INCORPORATED?
(12a) DATE OF INCORPORATION:
(13)LIST ALL BUSINESS LOCATIONS TO BE COVERED IN NEW YORK STATE:
/ /
(P.O. BOX IS NOT ACCEPTABLE AS A LOCATION. ONLY NEW YORK STATE LOCATIONS CAN BE COVERED.)
Address
City |
State |
Zip Code |
# of |
|
|
|
Employees |
|
NY |
|
|
NY
NY
Attach a separate sheet if additional space is needed.
(14) ADDITIONAL INFORMATION ON THE EMPLOYER(S) SEEKING COVERAGE, LISTED IN QUESTION (2):
Name of Employer
Federal Tax ID
NYS Unemployment ID
Attach a separate sheet if additional space is needed.
(15) WHAT IS THE NAME AND ADDRESS OF YOUR BANK?
Bank Name: |
|
|
Address: |
|
|
City: |
State: |
Zip Code: |
New York State Insurance Fund Workers’ Compensation and Employers’ Liability Application
Page 4 of 8
-
(16) INFORMATION ON THE PERSON YOU WISH US TO CONTACT FOR A PREMIUM AUDIT:
Name:
Address:
City:
Telephone:
Fax:
State:
Zip Code:
-
(17)PLEASE PROVIDE INFORMATION ON THE SOLE PROPRIETOR, ALL EXECUTIVE OFFICERS, PARTNERS, ELECTED OR APPOINTED OFFICIALS, OR MEMBERS OF GOVERNING BOARDS, IF APPLICABLE:
First Name :
Title:
Duties:
Address:
MI: Last Name:
Annual Salary:
City:
Telephone:
First Name :
Title:
Duties:
Address:
Fax:
State:
MI: Last Name:
Annual Salary:
Zip Code:
-
City:
Telephone:
First Name :
Title:
Duties:
Address:
Fax:
State:
MI: |
Last Name: |
|
|
Annual Salary: |
|
|
|
|
|
|
|
Zip Code:
-
City:
Telephone:
Attach a separate sheet if additional space is needed.
Fax:
State:
Zip Code:
-
New York State Insurance Fund Workers’ Compensation and Employers’ Liability Application
Page 5 of 8
(17a) ARE ANY OF THE INDIVIDUALS LISTED IN QUESTION (17) PARTNERS OR CORPORATE OFFICERS FOR A PARTNERSHIP OR
CORPORATION OTHER THAN THE EMPLOYER(S) SPECIFIED IN QUESTION (2)? |
YES |
NO |
(17b) IF YES, LIST THE NAME(S) OF ALL SUCH INDIVIDUALS WITH THEIR PRINCIPAL BUSINESS ADDRESS AND, FOR A CORPORATION, THE PERCENTAGE OF STOCK OWNERSHIP.
First Name:
Name of Partnership or Corporation:
Address:
City:
First Name:
Name of Partnership or Corporation:
MI: |
|
Last Name: |
|
|
|
% of Stock:
|
State: |
|
|
|
Zip Code: |
|
- |
||
|
|
|
|
|
|
|
|||
MI: |
|
|
Last Name: |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
% of Stock: |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address:
City:
State:
Zip Code:
-
Attach a separate sheet if additional space is needed.
(18) PLEASE PROVIDE INFORMATION ON YOUR DISABILITY BENEFITS INSURANCE:
Disability Benefits Carrier: |
|
|
Disability Policy Number: |
|
|
|
|
(18a) DO YOU WANT A DISABILITY BENEFITS INSURANCE QUOTE? |
YES |
||
(19) PLEASE PROVIDE INFORMATION ON YOUR GENERAL LIABILITY INSURANCE: |
|||
General Liability Insurance Carrier: |
|
General Liability Policy Number: |
|
NO
(20)HAVE YOU EVER BEEN IN BUSINESS UNDER A DIFFERENT NAME?
(20a) IF YES, PLEASE COMPLETE:
YES
NO
Name Used
Trade Name (if any)
Date Usage of Name was
Stopped or Changed
Attach a separate sheet if additional space is needed.
(21) IF YOU ARE INCORPORATED, HAVE THE PRINCIPALS OF THE CORPORATION PREVIOUSLY MANAGED A BUSINESS BY ANOTHER
NAME? |
YES |
NO |
(21a) IF YES, PLEASE COMPLETE:
Name Used
Trade Name (if any)
Date Usage of Name was
Stopped or Changed
Attach a separate sheet if additional space is needed.
New York State Insurance Fund Workers’ Compensation and Employers’ Liability Application
Page 6 of 8
(22)IS YOUR BUSINESS OR COMPANY AN AFFILIATE OR A SUBSIDIARY OF ANY OTHER COMPANY?
(22a) IF YES, PLEASE COMPLETE:
YES
NO
Name of Affiliate |
|
Relationship: |
|
|
||
or Subsidiary: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
||||
City: |
|
|
State: |
|||
|
|
|
|
|
|
|
Attach a separate sheet if additional space is needed. |
|
|
|
|
||
Present Workers’
Comp. Carrier:
Zip Code: |
- |
|
(23) ARE YOU ENGAGED IN ANY OTHER TYPE OF BUSINESS?
YES
NO
(23a) IF YES, PLEASE DESCRIBE OTHER BUSINESS OPERATIONS INCLUDING THE PRODUCTS AND SERVICES SOLD:
Business Description |
(Attach a separate sheet if additional space is needed.) |
|
|
(24)ARE
(24a) DO YOU LEASE EMPLOYEES TO OR FROM OTHER EMPLOYERS?
YES
YES
NO
NO
(25)PAYROLL VERIFICATION:
(This requirement does not apply to employers of domestic workers or to municipalities or other political subdivisions.)
At least one of the following items of payroll verification MUST accompany this application. Failure to provide payroll verification may result in rejection of your application for insurance. Please attach at least one of the following items to your application:
A copy of your previous insurance company’s premium audit bill showing the classifications and payrolls for the most recent policy period
Copies of Federal Tax Form 941 for the last four quarters
Copies of New York State Tax Form
If none of the foregoing documents are available because you are a new business or did not have employees, then check this box:
New York State Insurance Fund Workers’ Compensation and Employers’ Liability Application
Page 7 of 8

(26)I UNDERSTAND THAT THE INFORMATION WHICH I HAVE PROVIDED ON THIS APPLICATION WILL BE USED TO CALCULATE MY WORKERS’ COMPENSATION INSURANCE PREMIUM. I ALSO UNDERSTAND THAT I HAVE A CONTINUING OBLIGATION TO NOTIFY THE NEW YORK STATE INSURANCE FUND OF ANY CHANGES IN:
THE KINDS OF WORK WHICH THE BUSINESS IS DOING
THE SIZE OF OUR WORKFORCE
THE SIZE OF OUR PAYROLL
THE BUSINESS OWNERSHIP OR BUSINESS STRUCTURE
Print or Type Name of Owner, Partner or Officer:
Signature of Owner, Partner or Officer:
Date:
//
PLEASE PRINT, SIGN AND MAIL YOUR COMPLETED APPLICATION ALONG WITH THE REQUIRED DEPOSIT
Applicant, please note:
INFORMATION YOU PROVIDE IS PROTECTED BY THE PERSONAL PRIVACY PROTECTION LAW
The authority to obtain the personal information requested herein is found in Section 83 of the Workers’ Compensation Law as supplemented by Sections 450.1,
450.3and 450.5 of Chapter VI of Title 12( c ) of the Official Compilation of Codes, Rules and Regulations of the State of New York. The principal purpose for which the information is sought is to assist the New York State Insurance Fund in processing your insurance coverage with the New York State Insurance Fund and its release is governed by the limitations of the Personal Privacy Protection Law. This information will be maintained by the Director of Underwriting, New York State Insurance Fund, 199 Church Street, New York, NY 10007.
To ensure prompt service and processing, please mail your fully completed and signed application along with your deposit premium check and supporting documentation to:
NEW YORK STATE INSURANCE FUND DOCUMENT CONTROL CENTER – NEW BUSINESS 1 WATERVLIET AVENUE EXTENSION
ALBANY, NY 12206
For additional assistance, customer service and contact information:
Please visit our website at WWW.NYSIF.COM or telephone us at
New York State Insurance Fund Workers’ Compensation and Employers’ Liability Application
Page 8 of 8