The PDF editor which you'll take advantage of was made by our leading web developers. You can easily submit the ultimate health claim file instantly and without problems applying our application. Merely comply with this guide to begin with.
Step 1: Hit the orange "Get Form Now" button on this page.
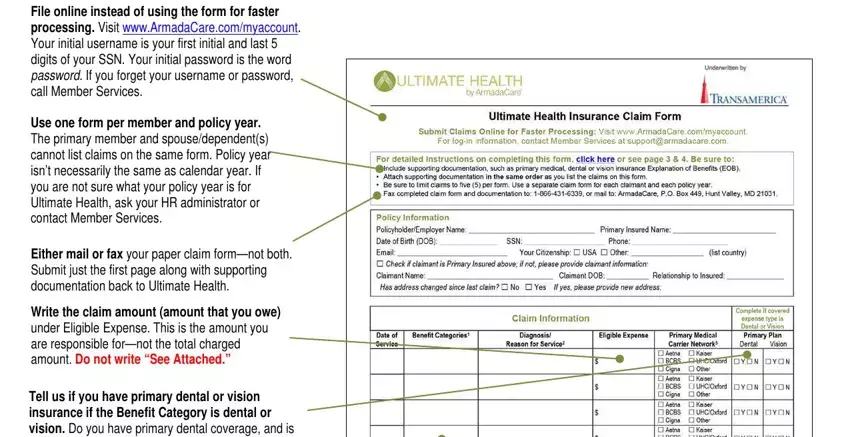
Step 2: The document editing page is now available. It's possible to add information or enhance existing information.
You should provide the following data so you can prepare the document:
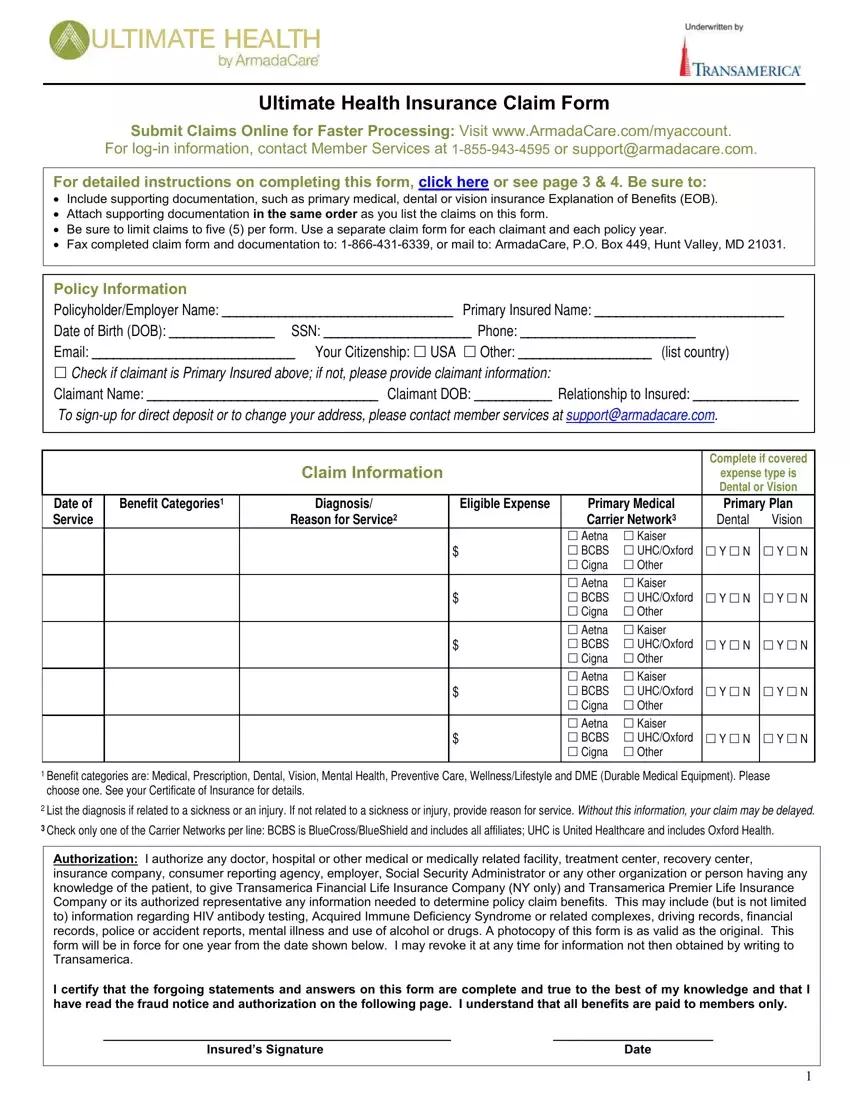
Please enter the essential information in the Diagnosis, Eligible, Expense Benefit, Categories Reason, for, Service Dental, Vision YN, YN YN, YN YN, YN and YN, YN field.
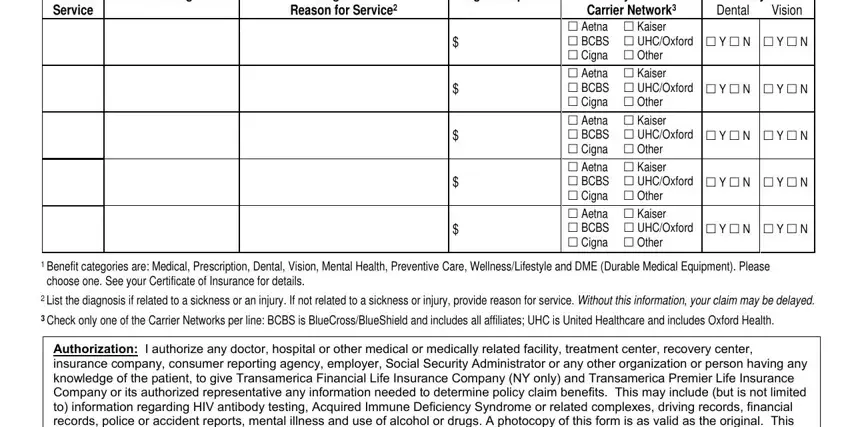
Put together the valuable details in the Insureds, Signature and Date section.

You'll need to indicate the rights and obligations of both parties in field .
Step 3: When you are done, press the "Done" button to upload the PDF form.
Step 4: To stay away from probable future issues, you should always possess around a pair of duplicates of each and every document.
