

universal medicine application form print can be filled out effortlessly. Just open FormsPal PDF tool to accomplish the job right away. To make our tool better and easier to use, we constantly implement new features, taking into consideration suggestions from our users. All it requires is a couple of simple steps:
Step 1: Just click on the "Get Form Button" at the top of this site to launch our pdf file editor. There you'll find everything that is needed to fill out your file.
Step 2: Using our advanced PDF editor, you can accomplish more than simply fill in blanks. Express yourself and make your documents seem faultless with customized textual content added, or adjust the original content to excellence - all comes with the capability to insert any pictures and sign it off.
As for the blank fields of this precise PDF, this is what you need to know:
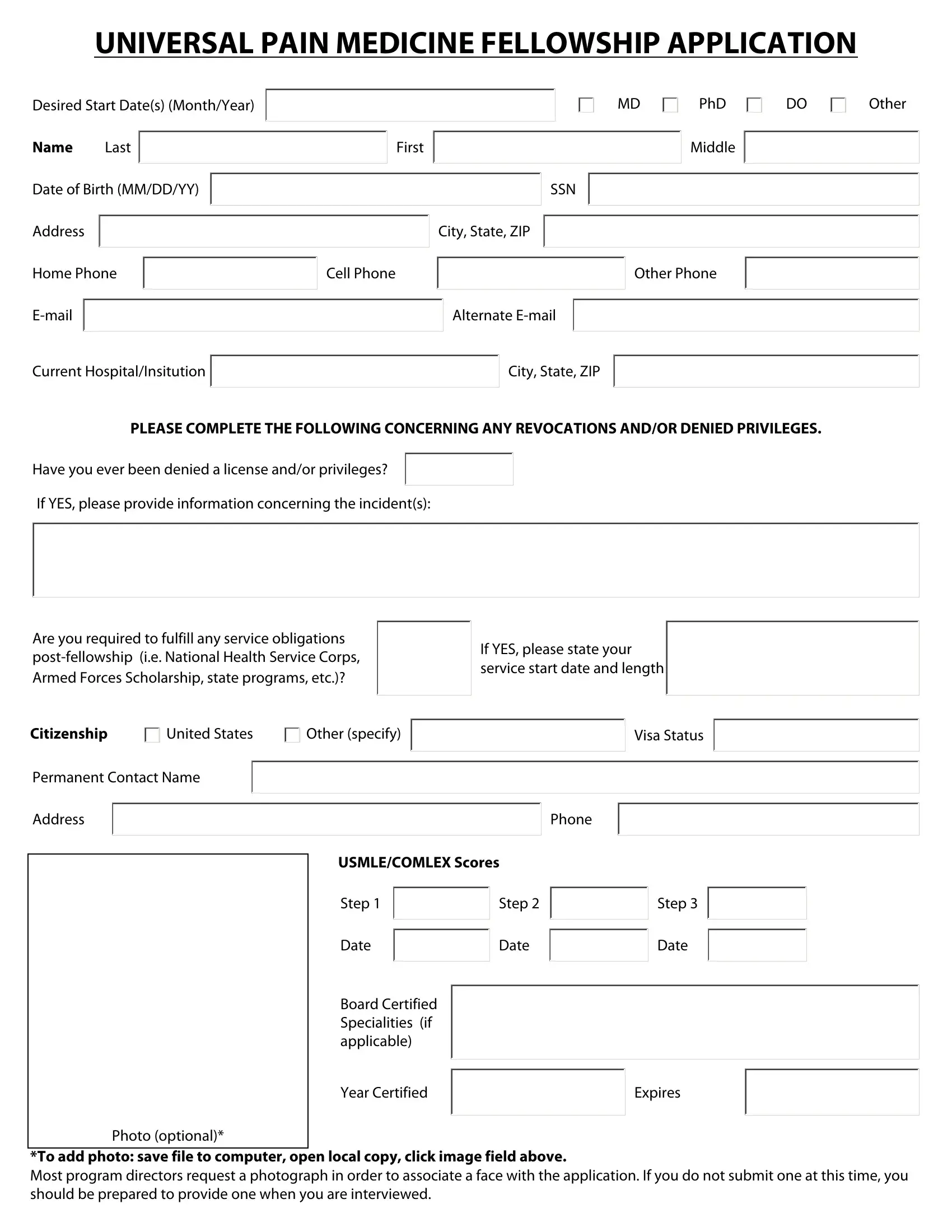
1. You should complete the universal medicine application form print accurately, therefore take care when filling out the segments that contain all these fields:
2. When the last array of blanks is completed, proceed to enter the suitable information in these - Have you ever been denied a, Are you required to fulfill any, If YES please state your service, Citizenship, United States, Other specify, Visa Status, Permanent Contact Name, Address, Phone, USMLECOMLEX Scores, Step, Step, and Step.
3. This part will be simple - fill in every one of the fields in Step, Date, Step, Date, Step, Date, Board Certified Specialities if, Year Certified, Expires, Photo optional, and To add photo save file to computer to complete this process.
4. The subsequent part comes next with all of the following blank fields to consider: Residency, Residency, Internship, Research Experience, ProgramHospital Name City State, Specialty, Dates MYMY, HonorsAwards, ProgramHospital Name City State, Type, Dates MYMY, Institution Name City State, Dates MYMY, HonorsAwards, and Research Topic.
5. Since you reach the end of your document, there are a couple extra requirements that need to be met. Notably, Research Experience, Institution Name City State, Dates MYMY, HonorsAwards, Research Topic, Duties, HonorsAwards, Institution Name City State, Degree, Dates MYMY, Medical School, and HonorsAwards should be done.
In terms of Degree and Dates MYMY, ensure that you review things here. These two are considered the most significant ones in the page.
Step 3: Soon after double-checking the completed blanks, click "Done" and you're good to go! Create a free trial plan at FormsPal and obtain immediate access to universal medicine application form print - available inside your FormsPal account. Here at FormsPal, we aim to be certain that all your information is maintained protected.