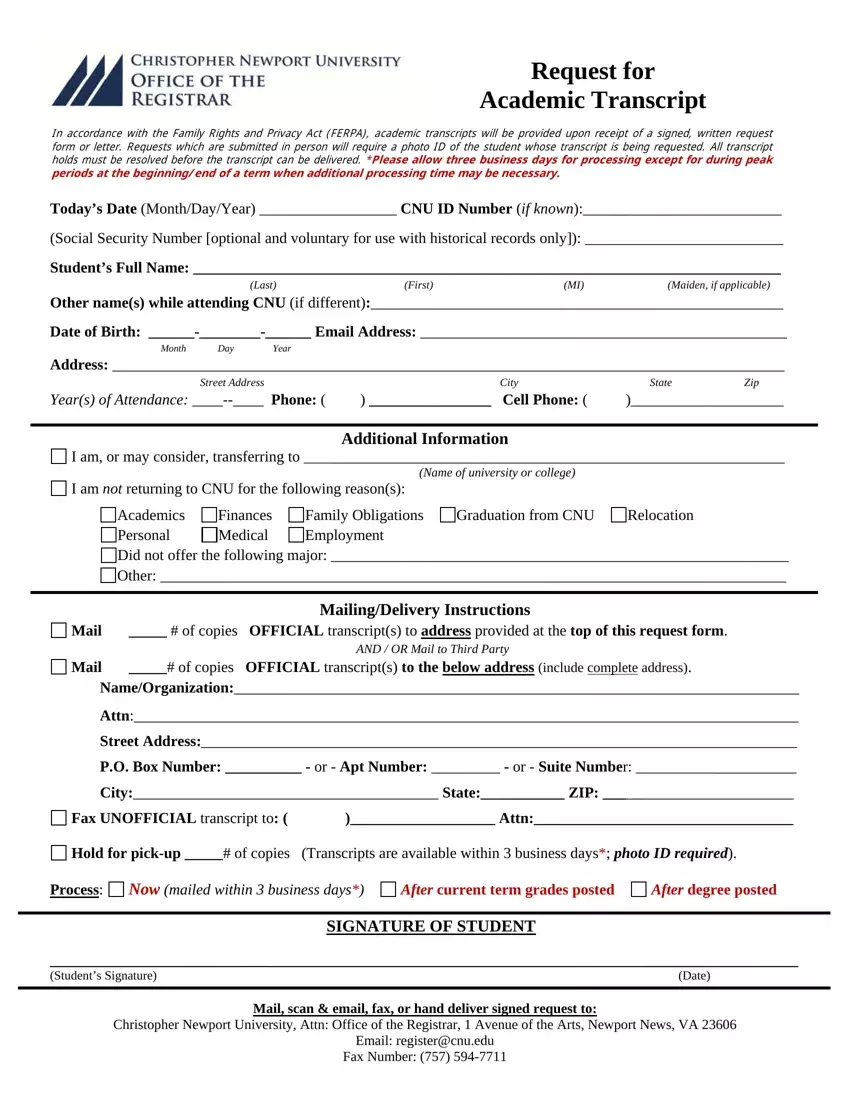
Request for
Academic Transcript
In accordance with the Family Rights and Privacy Act (FERPA), academic transcripts will be provided upon receipt of a signed, written request form or letter. Requests which are submitted in person will require a photo ID of the student whose transcript is being requested. All transcript holds must be resolved before the transcript can be delivered. *Please allow three business days for processing except for during peak periods at the beginning/end of a term when additional processing time may be necessary.
Today’s Date (Month/Day/Year) __________________ CNU ID Number (if known):__________________________
(Social Security Number [optional and voluntary for use with historical records only]): __________________________
Student’s Full Name: _____________________________________________________________________________
(Last)(First)(MI)(Maiden, if applicable)
Other name(s) while attending CNU (if different):______________________________________________________
Date of Birth: ______-________-______ Email Address: ________________________________________________
Month Day Year
Address: ________________________________________________________________________________________
Street Address |
City |
State |
Zip |
Year(s) of Attendance: ____--____ Phone: ( |
) ________________ Cell Phone: ( |
)____________________ |
Additional Information

 I am, or may consider, transferring to _______________________________________________________________
I am, or may consider, transferring to _______________________________________________________________
(Name of university or college)

 I am not returning to CNU for the following reason(s):
I am not returning to CNU for the following reason(s):
Academics |
Finances |
Family Obligations |
Graduation from CNU |
Relocation |
Personal |
Medical |
Employment |
|
|

 Did not offer the following major: ____________________________________________________________
Did not offer the following major: ____________________________________________________________

 Other: __________________________________________________________________________________
Other: __________________________________________________________________________________
Mailing/Delivery Instructions

 Mail _____ # of copies OFFICIAL transcript(s) to address provided at the top of this request form.
Mail _____ # of copies OFFICIAL transcript(s) to address provided at the top of this request form.
AND / OR Mail to Third Party

 Mail _____# of copies OFFICIAL transcript(s) to the below address (include complete address).
Mail _____# of copies OFFICIAL transcript(s) to the below address (include complete address).
Name/Organization:__________________________________________________________________________
Attn:_______________________________________________________________________________________
Street Address:______________________________________________________________________________
P.O. Box Number: __________ - or - Apt Number: _________ - or - Suite Number: _____________________
City:________________________________________ State:___________ ZIP: _________________________
|
|
|
|
Fax UNOFFICIAL transcript to: ( |
)___________________ Attn:__________________________________ |
Hold for pick-up _____# of copies (Transcripts are available within 3 business days*; photo ID required). |
Process: Now (mailed within 3 business days*) |
After current term grades posted |
After degree posted |
|
|
|
|
SIGNATURE OF STUDENT |
|
__________________________________________________________________________________________________
(Student’s Signature) |
(Date) |
|
|
Mail, scan & email, fax, or hand deliver signed request to:
Christopher Newport University, Attn: Office of the Registrar, 1 Avenue of the Arts, Newport News, VA 23606
Email: register@cnu.edu
Fax Number: (757) 594-7711