
usmepcom 680 can be completed online without difficulty. Simply open FormsPal PDF editor to finish the job in a timely fashion. In order to make our editor better and more convenient to use, we continuously implement new features, taking into account feedback from our users. By taking some simple steps, you may start your PDF journey:
Step 1: Simply click the "Get Form Button" at the top of this site to open our form editing tool. This way, you will find everything that is necessary to work with your file.
Step 2: With our handy PDF file editor, you can actually accomplish more than simply fill in forms. Try all of the functions and make your forms seem professional with customized textual content incorporated, or modify the file's original input to perfection - all comes with an ability to insert your own images and sign it off.
With regards to the blanks of this specific document, here's what you need to do:
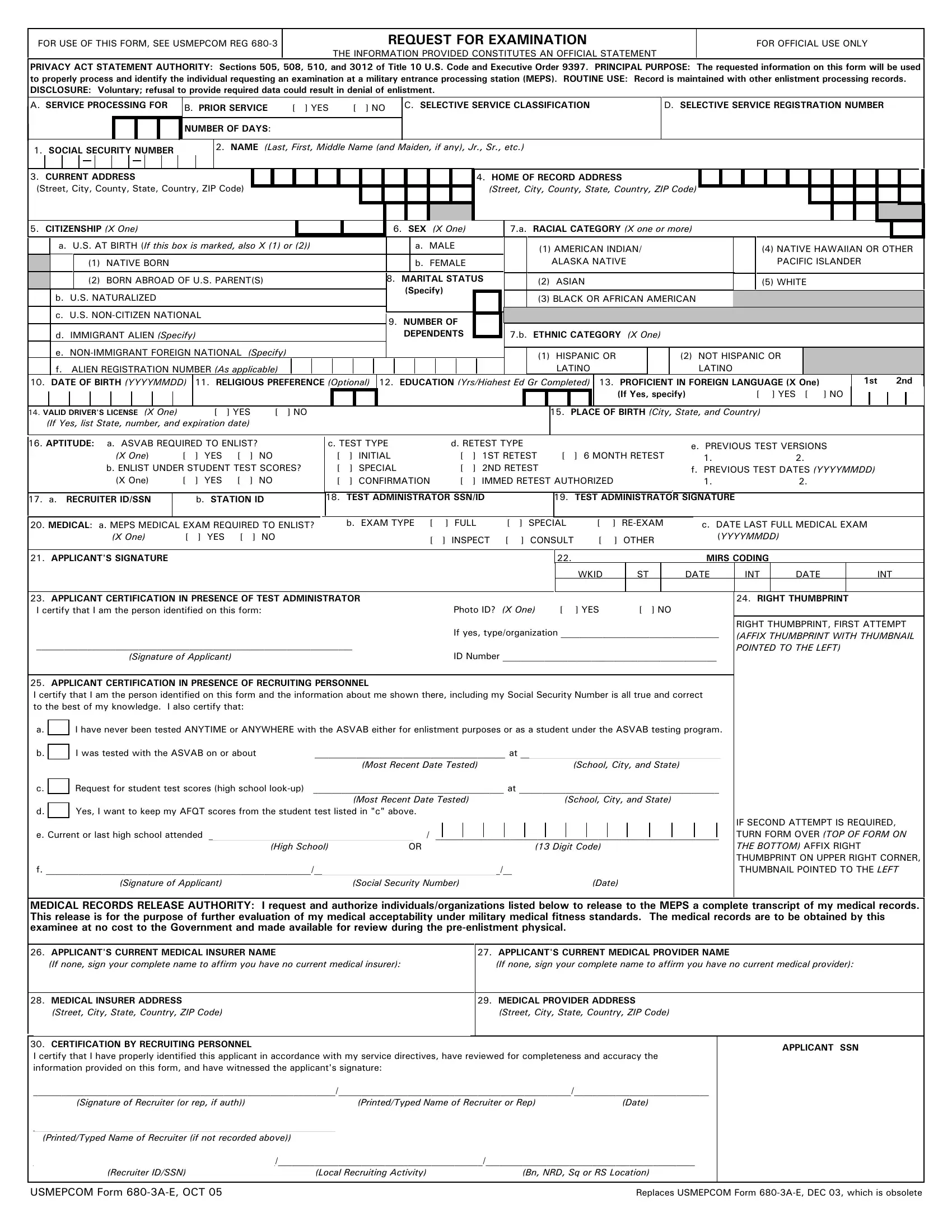
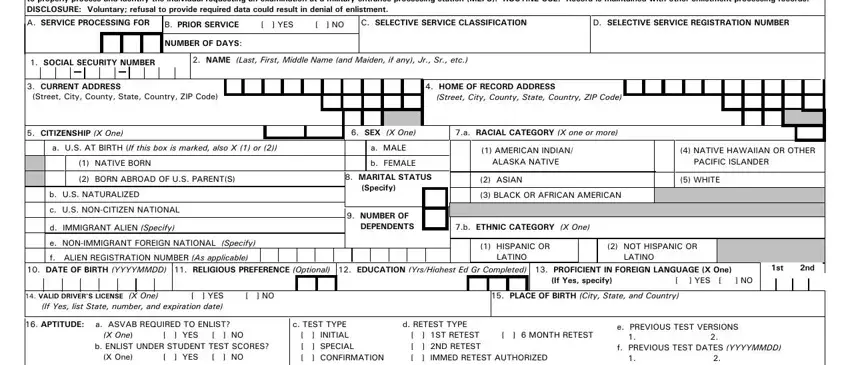
1. The usmepcom 680 requires specific details to be typed in. Be sure the subsequent blanks are completed:
2. Right after finishing this part, head on to the subsequent step and complete all required particulars in these blanks - a RECRUITER IDSSN, b STATION ID, c TEST TYPE INITIAL SPECIAL, TEST ADMINISTRATOR SIGNATURE, MEDICAL a MEPS MEDICAL EXAM, b EXAM TYPE FULL SPECIAL, INSPECT CONSULT OTHER, c DATE LAST FULL MEDICAL EXAM, APPLICANTS SIGNATURE, WKID, MIRS CODING ST, DATE, INT, DATE, and INT.
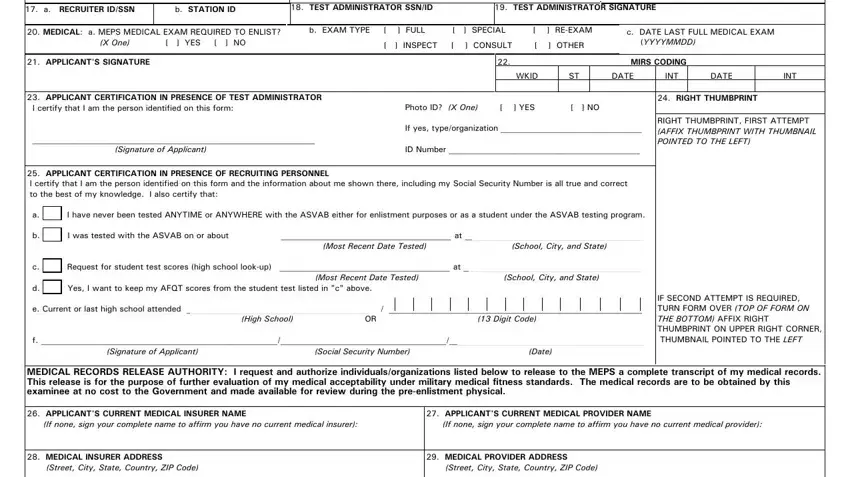
3. In this specific stage, look at CERTIFICATION BY RECRUITING, APPLICANT SSN, Signature of Recruiter or rep if, PrintedTyped Name of Recruiter or, PrintedTyped Name of Recruiter if, Recruiter IDSSN Local Recruiting, USMEPCOM Form AE OCT, and Replaces USMEPCOM Form AE DEC. These must be filled out with utmost awareness of detail.
When it comes to PrintedTyped Name of Recruiter or and PrintedTyped Name of Recruiter if, be certain that you get them right in this current part. Those two are the most important fields in this PDF.
Step 3: Ensure your details are accurate and then click on "Done" to complete the task. Right after setting up a7-day free trial account with us, you will be able to download usmepcom 680 or send it through email right away. The document will also be accessible in your personal account with your every single edit. Here at FormsPal.com, we strive to make sure your details are kept protected.