
With the online PDF tool by FormsPal, you may fill in or modify usps postalease here. Our tool is continually evolving to deliver the best user experience achievable, and that is thanks to our dedication to constant improvement and listening closely to customer comments. To get the ball rolling, go through these basic steps:
Step 1: Simply hit the "Get Form Button" at the top of this webpage to access our pdf file editor. There you'll find everything that is needed to fill out your file.
Step 2: With this handy PDF file editor, you can actually do more than merely complete forms. Edit away and make your docs seem great with custom text added in, or optimize the file's original content to excellence - all that comes with the capability to incorporate almost any photos and sign it off.
Be attentive while completing this pdf. Make certain all necessary fields are done accurately.
1. Firstly, while filling in the usps postalease, start in the part with the next fields:
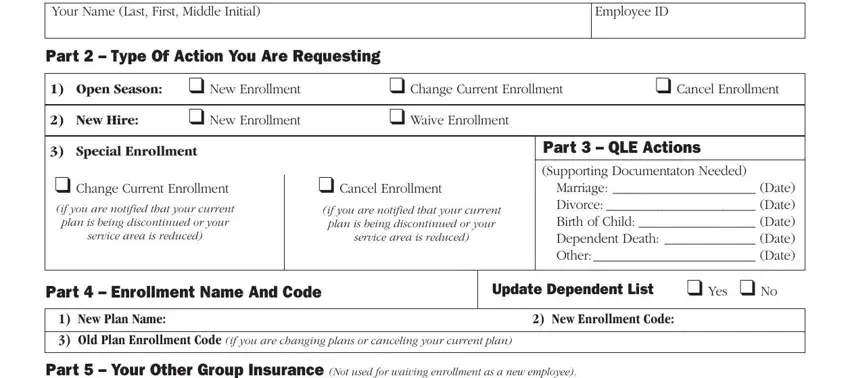
2. Just after filling out the previous step, go on to the subsequent stage and fill out all required details in these fields - Your Name Last First Middle, Part Type Of Action You Are, OpenSeason New Enrollment, Change Current Enrollment, Cancel Enrollment, NewHire, New Enrollment, Waive Enrollment, SpecialEnrollment, Change Current Enrollment if you, plan is being discontinued or your, service area is reduced, Cancel Enrollment, if you are notified that your, and plan is being discontinued or your.
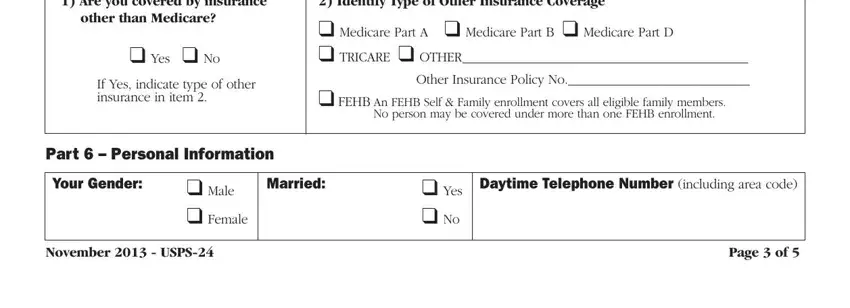
3. Your next step is generally straightforward - fill in all of the fields in Areyoucoveredbyinsurance, otherthanMedicare, Yes No, If Yes indicate type of other, Medicare Part A Medicare Part B, FEHB An FEHB Self Family, No person may be covered under, Part Personal Information, Your Gender, Married, Male Female, Yes No, Daytime Telephone Number including, NovemberUSPS, and Pageof to conclude the current step.
Be really attentive while filling out If Yes indicate type of other and Married, as this is where many people make mistakes.
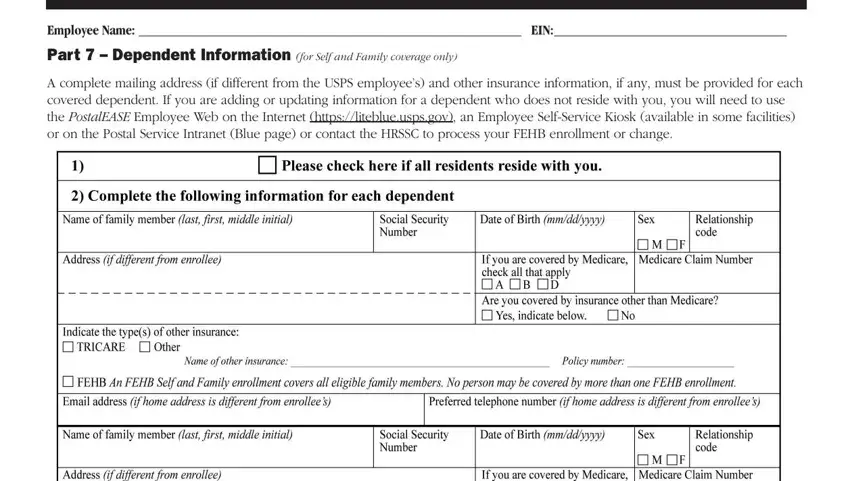
4. Filling in EmployeeName EIN, Part Dependent Information for, and A complete mailing address if is crucial in this fourth part - ensure to be patient and take a close look at each blank area!
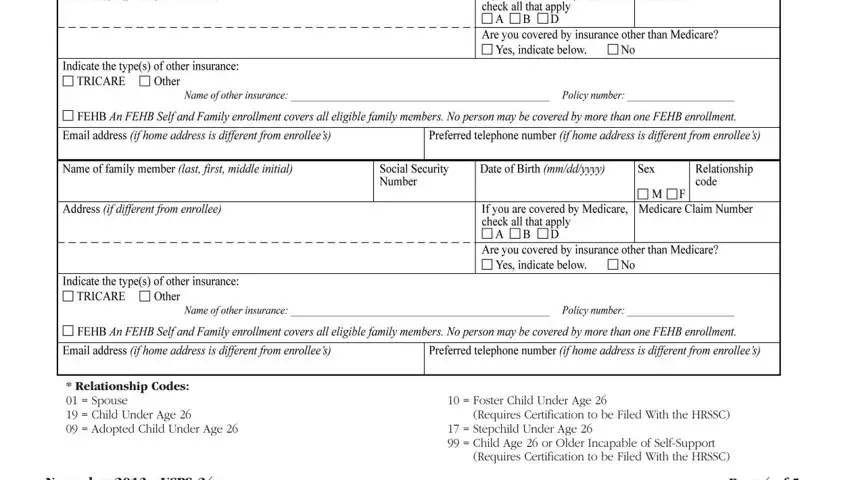
5. To finish your form, the last section features a few extra blank fields. Entering RelationshipCodes Spouse Child, Foster Child Under Age, Requires Certification to be Filed, Stepchild Under Age Child Age, Requires Certification to be Filed, NovemberUSPS, and Pageof should wrap up everything and you will be done in a tick!
Step 3: As soon as you have glanced through the details provided, simply click "Done" to finalize your form at FormsPal. Grab the usps postalease once you sign up for a 7-day free trial. Conveniently get access to the pdf document in your FormsPal account, together with any modifications and adjustments automatically preserved! FormsPal guarantees secure document tools with no data recording or distributing. Rest assured that your details are safe here!