
Using the online PDF editor by FormsPal, you'll be able to fill out or edit myeloma here and now. Our editor is constantly developing to deliver the best user experience attainable, and that is due to our resolve for continuous enhancement and listening closely to comments from users. With a few easy steps, it is possible to start your PDF journey:
Step 1: Press the "Get Form" button at the top of this page to access our editor.
Step 2: With this advanced PDF editor, you can do more than merely fill out blank fields. Edit away and make your docs look perfect with customized textual content added in, or optimize the file's original content to excellence - all comes with an ability to incorporate almost any pictures and sign the document off.
If you want to finalize this form, ensure that you provide the information you need in every single blank:
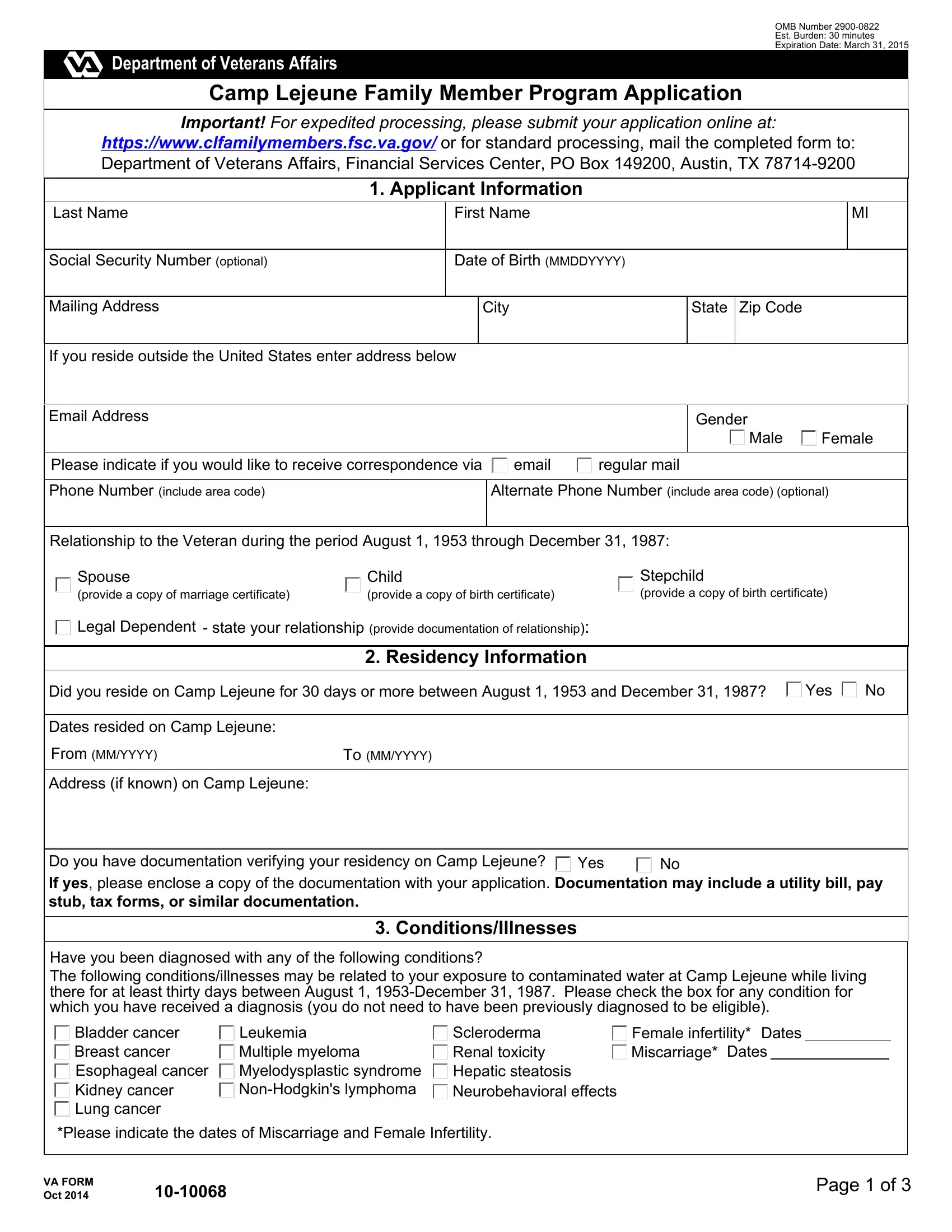
1. To start off, once filling in the myeloma, beging with the page with the next blank fields:
2. Once your current task is complete, take the next step – fill out all of these fields - Spouse provide a copy of marriage, Child provide a copy of birth, Stepchild provide a copy of birth, Legal Dependent state your, Residency Information, Did you reside on Camp Lejeune for, Yes, Dates resided on Camp Lejeune, From MMYYYY, To MMYYYY, Address if known on Camp Lejeune, Do you have documentation, Yes, Have you been diagnosed with any, and ConditionsIllnesses with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
It's easy to get it wrong when filling out your From MMYYYY, hence make sure that you reread it before you'll send it in.
3. This next step will be focused on Bladder cancer Breast cancer, Leukemia Multiple myeloma, Scleroderma Renal toxicity Hepatic, Please indicate the dates of, VA FORM Oct, and Page of - complete all of these blanks.

4. Your next paragraph needs your details in the subsequent places: Do you have health care coverage, Yes, Health Care Coverage, Medicare Part A, Medicare Part B, Effective Date MMDDYYYY, Effective Date MMDDYYYY, Medicare Advantage, Effective Date MMDDYYYY, Medicare Part D, Effective Date MMDDYYYY, MedicaidState Assistance, Effective Date MMDDYYYY, TRICARE, and CHAMPVA. Be sure to give all needed information to move onward.
5. The last section to conclude this form is critical. Be sure you fill out the required blanks, which includes Does your health care coverage, Last Name, Veteran Information, First Name, Social Security Number optional, Phone Number include area code, Date of Birth MMDDYYYY, Is Veteran deceased No, Yes, Gender, Male, Female, Dates Stationed at Camp Lejeune If, List Units and Ranks while, and From MMYYYY, prior to using the form. If you don't, it can end up in a flawed and possibly nonvalid paper!
Step 3: Before obtaining the next stage, check that blank fields were filled in correctly. As soon as you establish that it's correct, click “Done." After setting up afree trial account here, it will be possible to download myeloma or send it through email right away. The document will also be accessible through your personal account with your each modification. We don't share or sell the information you type in while filling out forms at our website.