The champva 10 10d form printable filling out procedure is very simple. Our editor enables you to use any PDF form.
Step 1: You can choose the orange "Get Form Now" button at the top of the following webpage.
Step 2: So, you can update the champva 10 10d form printable. The multifunctional toolbar allows you to add, remove, adapt, highlight, and also conduct similar commands to the words and phrases and areas inside the file.
Fill out all of the following sections to create the form:
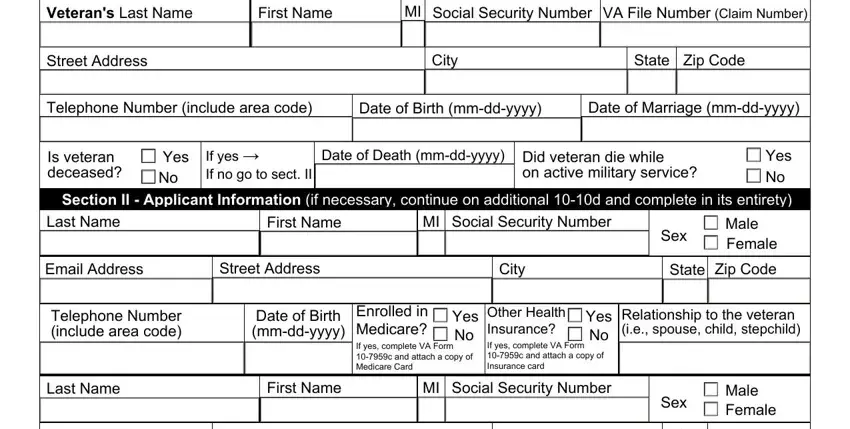
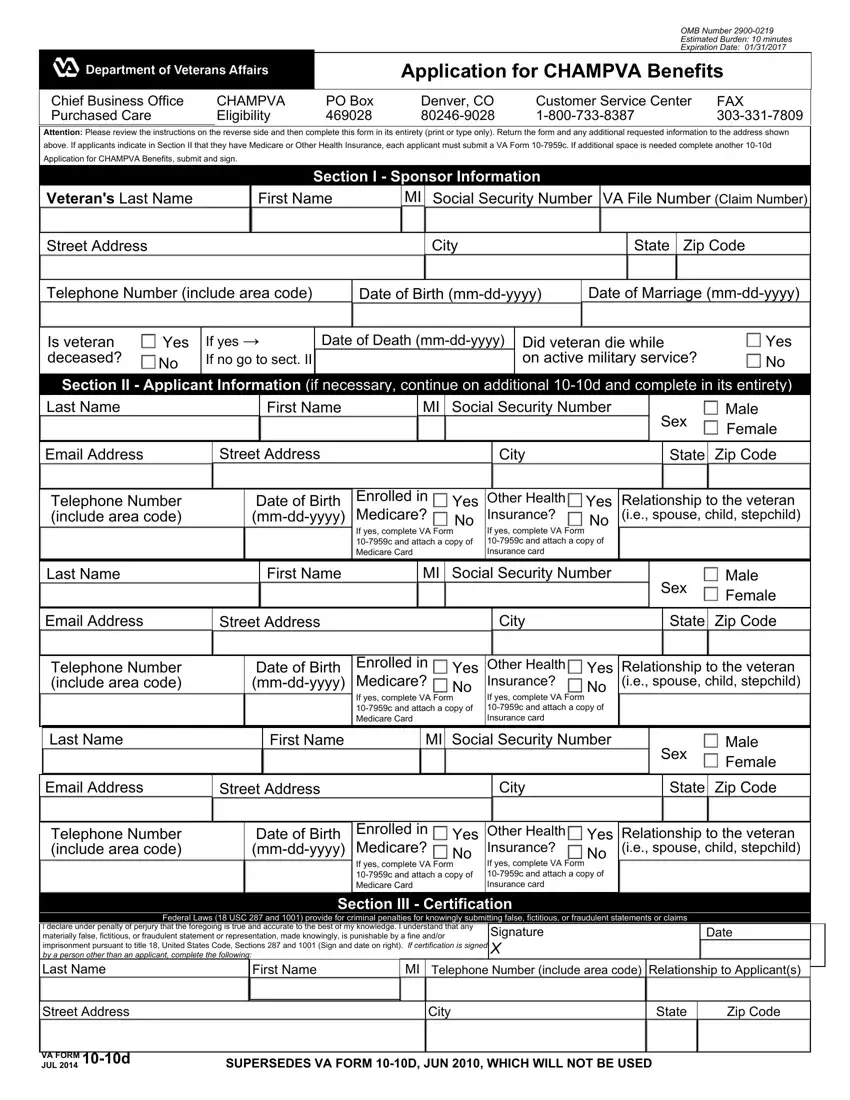
Within the field Email Address, Street Address, City, State Zip Code, Telephone Number include area code, Date of Birth mmddyyyy, Enrolled in Medicare If yes, Yes Other Health No, Yes Relationship to the veteran ie, Last Name, First Name, MI Social Security Number, Email Address, Street Address, and City write down the data which the application requests you to do.
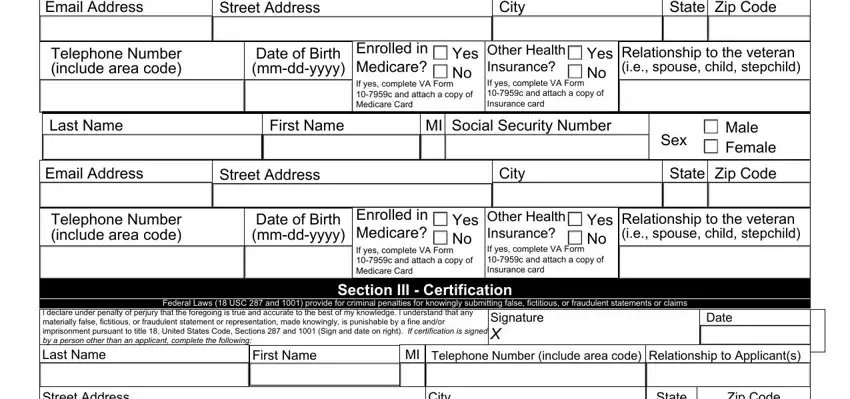
You will be expected to write down the details to let the platform fill out the area Street Address, VA FORM, JUL d, City, State, Zip Code, and SUPERSEDES VA FORM D JUN WHICH.

The Privacy Act Information The, The Paperwork Reduction Act This, Application for CHAMPVA Benefits, CHAMPVA Eligibility Criteria, The following persons are eligible, the spouse or child of a veteran, and permanent and total section has to be applied to list the rights or responsibilities of both parties.
Fill out the template by analyzing the following areas: Spouse Refers to a person who is, Child Includes legitimate adopted, NOTE Except for stepchildren the, School Certification, and In order to extend CHAMPVA.
Step 3: Choose "Done". Now you may upload the PDF form.
Step 4: Just be sure to create as many copies of the document as you can to remain away from possible issues.
