The PDF editor you will take advantage of was created by our top web developers. It is possible to create the Va Form 10 10Ez form instantly and effortlessly applying our app. Simply stick to this guide to start out.
Step 1: Find the button "Get Form Here" on this website and select it.
Step 2: Right now, you can start editing your Va Form 10 10Ez. The multifunctional toolbar is readily available - add, eliminate, modify, highlight, and undertake other commands with the content in the form.
In order to obtain the file, enter the details the program will request you to for each of the next sections:
In the TYPE OF BENEFITS APPLYING FOR, ENROLLMENT VA Medical Benefits, REGISTRATION VA Health Services, A VETERANS NAME Last First Middle, B PREFERRED NAME, MOTHERS MAIDEN NAME, A BIRTH SEX, B SELFIDENTIFIED GENDER IDENTITY, MALE, MALE, FEMALE, FEMALE, TRANSMALETRANSMANFEMALETOMALE, TRANSFEMALETRANSWOMANMALETOFEMALE, and CHOOSE NOT TO ANSWER box, note your data.
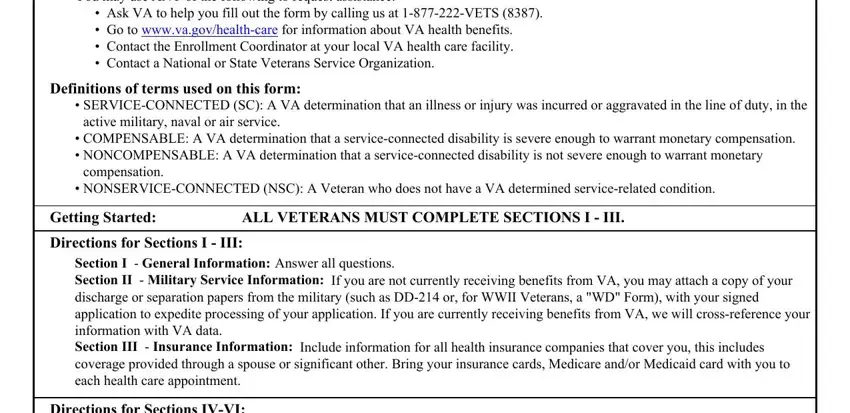
You can be required to write down the particulars to help the program fill out the area DESIGNEE INDIVIDUAL TO RECEIVE, WHICH VA MEDICAL CENTER OR, WOULD YOU LIKE FOR VA TO CONTACT, for listing of facilities visit, APPOINTMENT, YES, A LAST BRANCH OF SERVICE, B LAST ENTRY DATE mmddyyyy, C FUTURE DISCHARGE DATE mmddyyyy, D LAST DISCHARGE DATE mmddyyyy, SECTION II MILITARY SERVICE, E DISCHARGE TYPE, F MILITARY SERVICE NUMBER, MILITARY HISTORY Check yes or no, and YES.
The APPLICATION FOR HEALTH BENEFITS, VETERANS NAME Last First Middle, SOCIAL SECURITY NUMBER, ENTER YOUR HEALTH INSURANCE, SECTION III INSURANCE INFORMATION, NAME OF POLICY HOLDER, POLICY NUMBER, GROUP CODE, ARE YOU ELIGIBLE FOR MEDICAID, Federal health insurance for low, YES, A ARE YOU ENROLLED IN MEDICARE, YES, B EFFECTIVE DATE mmddyyyy, and SPOUSES NAME Last First Middle area needs to be used to list the rights or responsibilities of both sides.
End by looking at the next fields and preparing them as needed: E SPOUSES ADDRESS AND TELEPHONE, if different from Veterans, IF YOUR SPOUSE OR DEPENDENT CHILD, YEAR DID YOU PROVIDE SUPPORT, YES, F IF CHILD IS BETWEEN AND YEARS, SCHOOL LAST CALENDAR YEAR, YES, G EXPENSES PAID BY YOUR DEPENDENT, VOCATIONAL REHABILITATION OR, A VETERANS EMPLOYMENT STATUS Check, B DATE OF RETIREMENT mmddyyyy, FULL TIME, PART TIME, and NOT EMPLOYED.
Step 3: Choose the Done button to assure that your finished form may be exported to any kind of electronic device you end up picking or mailed to an email you specify.
Step 4: In order to prevent possible forthcoming complications, be sure to have as much as a couple of copies of each and every file.
