
 UNKNOWN
UNKNOWN
 U.S. CITIZEN BY BIRTH
U.S. CITIZEN BY BIRTH
 NO
NO
 NO
NO
 NO
NO
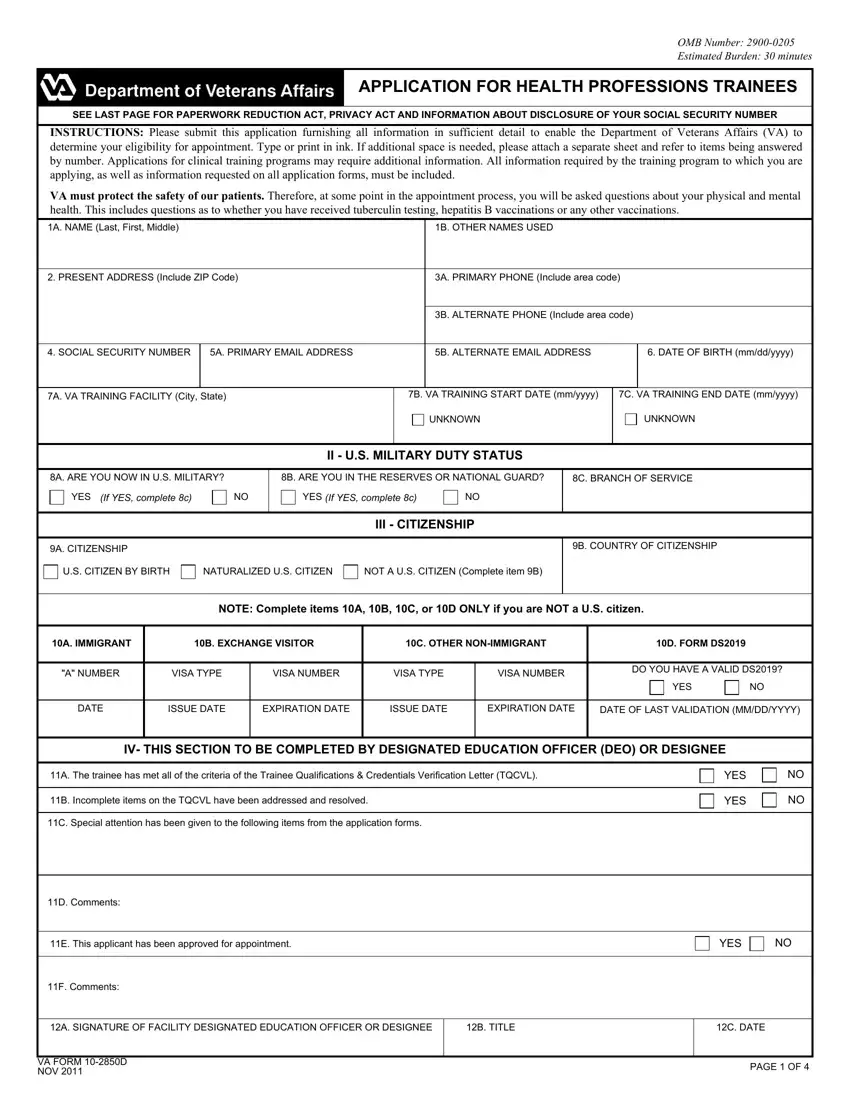
The idea driving our PDF editor was to ensure it is as simple as it can be. You'll find the entire process of filling up va health professions trouble-free as soon as you keep to all of these steps.
Step 1: On this website page, press the orange "Get form now" button.
Step 2: At the moment, you may change your va health professions. This multifunctional toolbar allows you to insert, remove, change, highlight, and undertake other commands to the text and fields inside the document.
Create the va health professions PDF by providing the content necessary for each individual area.
Type in the demanded data in the area A NUMBER, VISA TYPE, VISA NUMBER, VISA TYPE, VISA NUMBER, DO YOU HAVE A VALID DS, YES, DATE, ISSUE DATE, EXPIRATION DATE, ISSUE DATE, EXPIRATION DATE, DATE OF LAST VALIDATION MMDDYYYY, IV THIS SECTION TO BE COMPLETED BY, and A The trainee has met all of the.
You should point out the crucial information within the LAST NAME FIRST NAME MIDDLE NAME, SOCIAL SECURITY NUMBER, V LICENSE CERTIFICATION OR, A LIST ALL LICENSES, B STATE ISSUING LICENSE, C LICENSE CERTIFICATION OR, D EXPIRATION DATE MMDDYYYY, VI LICENSE CERTIFICATION OR, A LIST ALL LICENSES CERTIFICATIONS, B STATE ISSUING LICENSE, C LICENSE CERTIFICATION OR, D EXPIRATION DATE MMDDYYYY, and ENTER YOUR NATIONAL PROVIDER section.
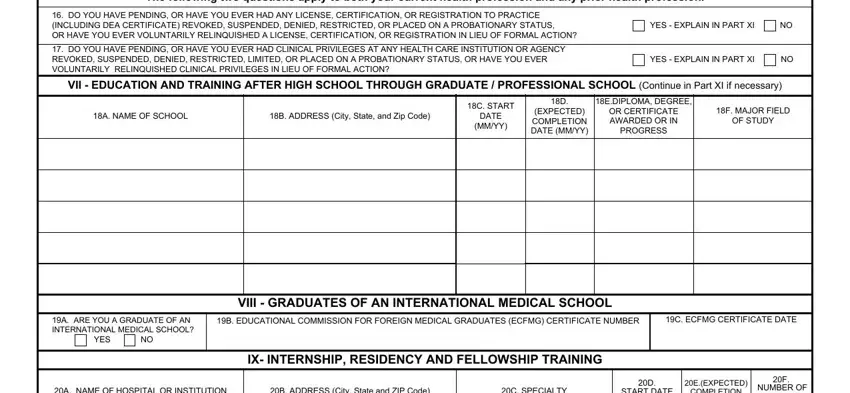
The The following two questions apply, DO YOU HAVE PENDING OR HAVE YOU, DO YOU HAVE PENDING OR HAVE YOU, YES EXPLAIN IN PART XI, YES EXPLAIN IN PART XI, VII EDUCATION AND TRAINING AFTER, A NAME OF SCHOOL, B ADDRESS City State and Zip Code, C START DATE MMYY, D EXPECTED COMPLETION DATE MMYY, EDIPLOMA DEGREE OR CERTIFICATE, F MAJOR FIELD OF STUDY, A ARE YOU A GRADUATE OF AN, YES, and VIII GRADUATES OF AN box will be your place to put the rights and obligations of either side.
Check the fields A NAME OF HOSPITAL OR INSTITUTION, B ADDRESS City State and ZIP Code, C SPECIALTY, D START DATE MMYY, EEXPECTED COMPLETION DATE MMYY, F NUMBER OF MONTHS COMPLETED, VA FORM D NOV, and PAGE OF and then fill them in.
Step 3: As you hit the Done button, your finished file can be simply exported to all of your devices or to electronic mail specified by you.
Step 4: Just be sure to make as many copies of the document as you can to prevent possible complications.
