VA Form 10-5345, titled “Request for and Authorization to Release Medical Records or Health Information,” allows veterans to authorize the release of their medical records and health information to external entities, such as private health care providers, insurance companies, or legal representatives. This form is particularly important for ensuring continuity of care when a veteran receives medical treatment outside the VA system or when records are needed for personal, insurance, or legal purposes. By completing VA Form 10-5345, veterans facilitate the secure and efficient transfer of their health information, respecting privacy laws and ensuring that their health data is handled appropriately.
Other VA Forms
If you’d like to find more VA PDFs you can edit and fill in online, listed here are examples of the more popular forms among our users. Also, do not forget that you can actually upload, fill out, and edit any PDF form at FormsPal.
First of all, you need to find a proper VA form. The one presented on the website of the US Department of Veteran Affairs might be your form to choose. Or you can avoid searching the internet and use the VA form that you can find on our website. After you download the form, you have to thoroughly read the Privacy Act at the beginning of the document, which touches on the ethos of using VA forms.
Then, you can start filling in the information about the patient, authorized people or organizations, and the type of information to be released.
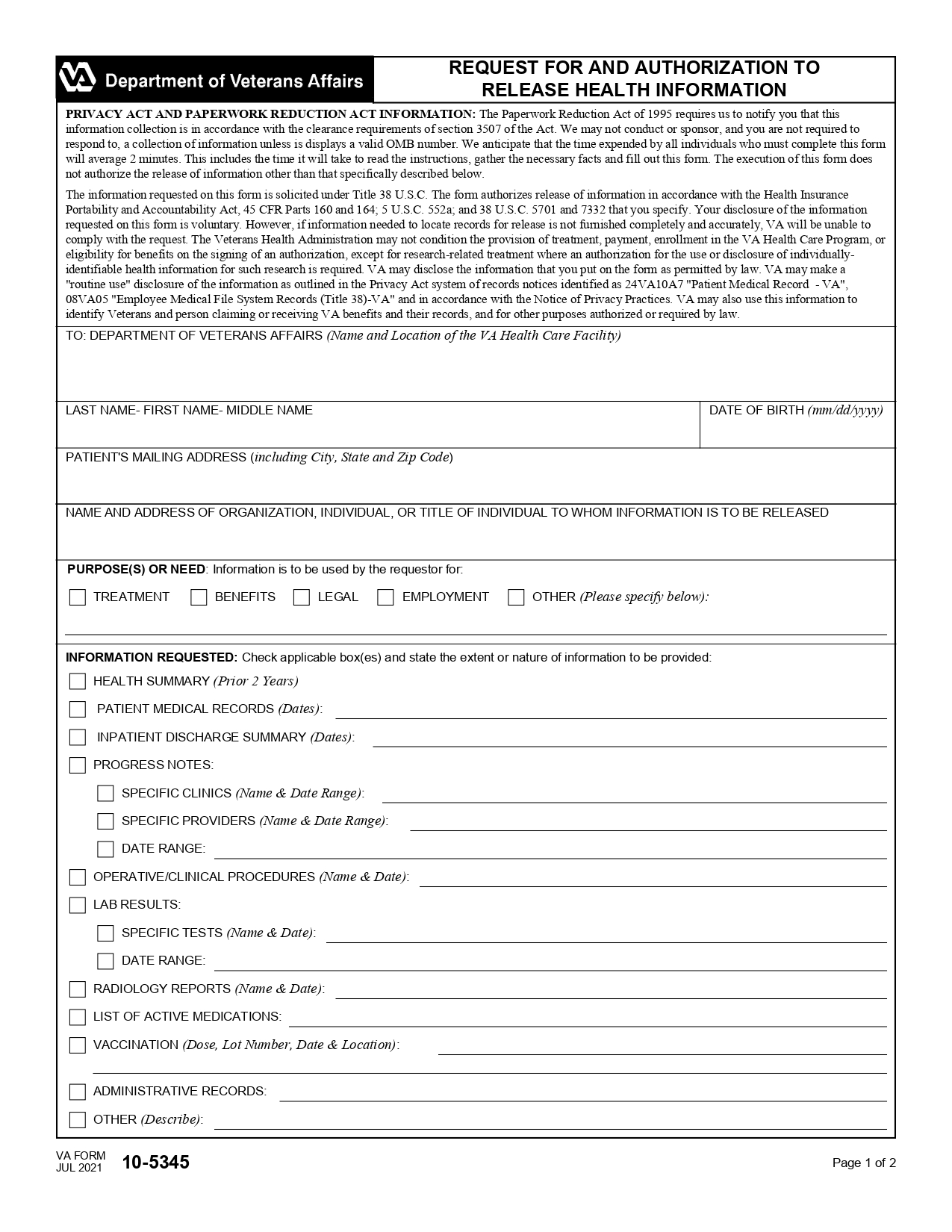
Step 1 – The patient’s information
The first information to include in the form is the name and address of the healthcare facility. Then, include the name and address of the patient plus their mailing address.
Step 2 – Persons/entities who will get access to the information
Next, the name of the organization to which the information will be disclosed should be mentioned. If the patient wishes to authorize individuals to access their medical records, the names of those people plus their titles should be written.
Step 3 – The purpose
The purpose of releasing information is what should be included next. It might tell that the information will be used by the requestor for treatment, to provide health benefits, for employment purposes, etc.
Step 4 – What information is requested
When using the form provided by the US Department of Veteran Affairs, one will have to check the boxes with the data that the patient wants to release. The duration of the release should be provided in front of each of the chosen boxes.
Step 5 – Sensitive diagnoses
The next section should touch on the release of the information regarding non-treatment purposes. It includes information about drug or alcohol abuse, HIV, etc.
Step 6 – Authorization
The patient should carefully read the Authorization section with the information about the revocation of the authorizations and other important aspects of using the form.
Step 7 – Expiration
The document should include the information on the date when it will automatically expire.
Step 8 – Signatures
The last step is to put the patient’s signature. If the patient is unable to sign the document, their legal representative’s signature and relation to the patient need to be included. The date of signing the document should be written down as well.
There will be the only section in the document that should be left blank. It is the last section of the document that is filled by the Veterans Administration.