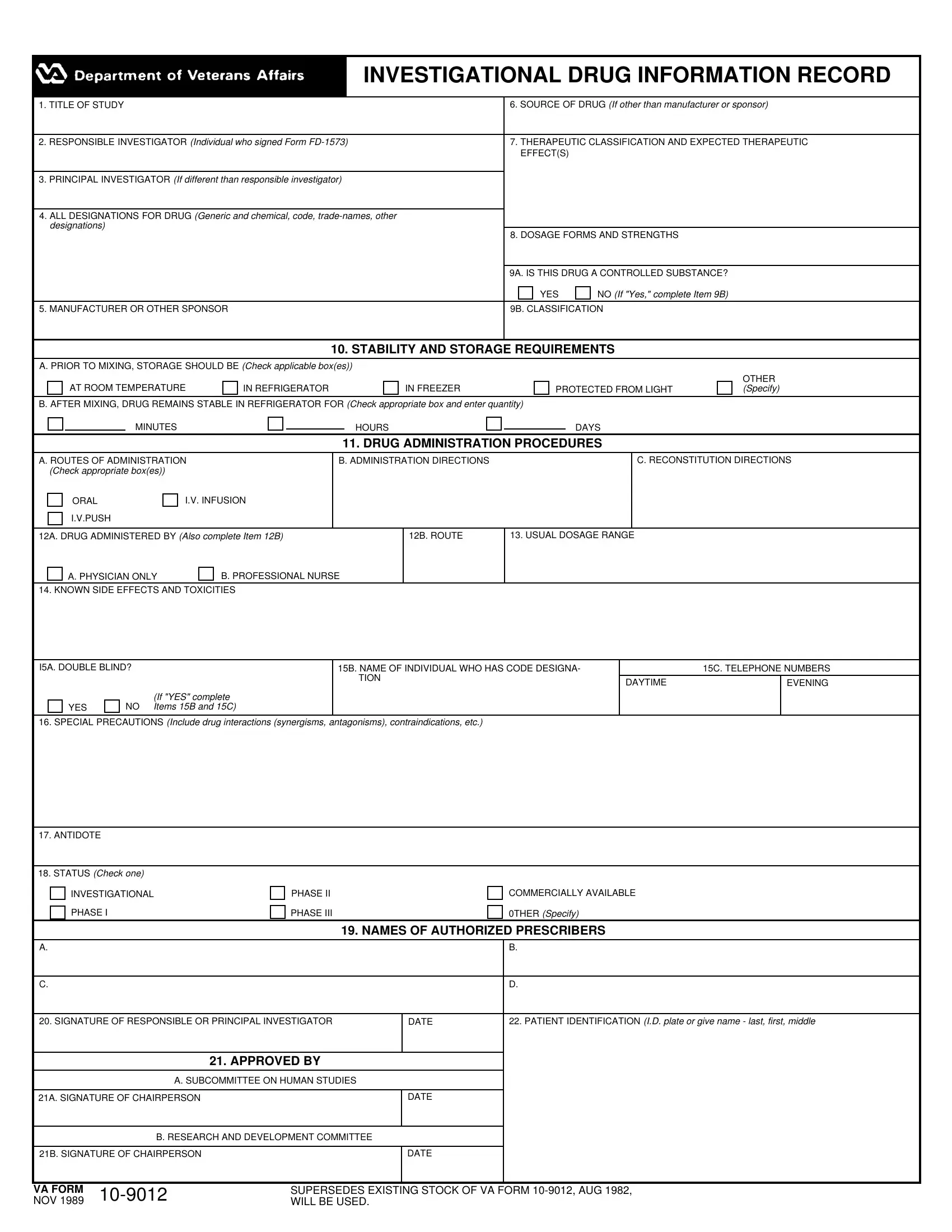
Navigating through the maze of paperwork in medical research, one encounters the VA Form 10-9012, a critical document for those involved in investigational drug studies. This form, known as the Investigational Drug Information Record, functions as a comprehensive tool for documenting the essential details of a drug under investigation. From the study's title to the intricate details about the drug’s administration, dosage, and storage requirements, the form ensures every facet is meticulously recorded. It covers who’s responsible for the investigation, the drug's source if it's not from the manufacturer, and the drug's therapeutic classification and expected effects. More than just a formality, VA Form 10-9012 delves into the specifics of dosage forms, strengths, stability, administration procedures, and even the handling of controlled substances. Additionally, it touches on vital safety aspects, such as known side effects, toxicities, special precautions, and the antidote for adverse reactions, if available. The form also notes the investigational phase of the drug and lists authorized prescribers, underscoring its role in bridging experimental therapies with patient care. By keeping a detailed record, this form ensures that investigational drugs are handled safely and effectively, marking a significant step in the journey from research to real-world application.
| Question | Answer |
|---|---|
| Form Name | Va Form 10 9012 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | responsible investigational 12b form, va 10 9012, 9012 form, drug information record |
|
|
|
|
INVESTIGATIONAL DRUG INFORMATION RECORD |
|
|
|
|
|
|
1. TITLE OF STUDY |
6. SOURCE OF DRUG (If other than manufacturer or sponsor) |
||
|
|
|
||
|
2. RESPONSIBLE INVESTIGATOR (Individual who signed Form |
7. THERAPEUTIC CLASSIFICATION AND EXPECTED THERAPEUTIC |
||
|
|
|
|
EFFECT(S) |
3.PRINCIPAL INVESTIGATOR (If different than responsible investigator)
4.ALL DESIGNATIONS FOR DRUG (Generic and chemical, code,
8. DOSAGE FORMS AND STRENGTHS
9A. IS THIS DRUG A CONTROLLED SUBSTANCE?
YES |
|
NO (If "Yes," complete Item 9B) |
5. MANUFACTURER OR OTHER SPONSOR |
9B. CLASSIFICATION |
10.STABILITY AND STORAGE REQUIREMENTS
A.PRIOR TO MIXING, STORAGE SHOULD BE (Check applicable box(es))
AT ROOM TEMPERATURE
IN REFRIGERATOR
IN FREEZER
PROTECTED FROM LIGHT
OTHER (Specify)
B. AFTER MIXING, DRUG REMAINS STABLE IN REFRIGERATOR FOR (Check appropriate box and enter quantity)
|
|
MINUTES |
|
|
|
HOURS |
|
DAYS |
||
|
|
|
|
|
|
|||||
|
|
|
|
|
11. DRUG ADMINISTRATION PROCEDURES |
|||||
|
|
|
|
|
|
|
|
|
|
|
A. ROUTES OF ADMINISTRATION |
|
B. ADMINISTRATION DIRECTIONS |
|
|
C. RECONSTITUTION DIRECTIONS |
|||||
(Check appropriate box(es)) |
|
|
|
|
|
|
|
|
||
|
ORAL |
I.V. INFUSION |
|
|
|
|
|
|
|
|
|
I.V.PUSH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12A. DRUG ADMINISTERED BY (Also complete Item 12B) |
|
|
|
12B. ROUTE |
13. USUAL DOSAGE RANGE |
|||||
|
A. PHYSICIAN ONLY |
B. PROFESSIONAL NURSE |
|
|
|
|
||||
14. KNOWN SIDE EFFECTS AND TOXICITIES
I5A. DOUBLE BLIND? |
|
15B. NAME OF INDIVIDUAL WHO HAS CODE DESIGNA- |
|
15C. TELEPHONE NUMBERS |
||
|
|
|
TION |
DAYTIME |
|
EVENING |
|
|
|
|
|
||
|
|
(If "YES" complete |
|
|
|
|
YES |
NO |
Items 15B and 15C) |
|
|
|
|
16.SPECIAL PRECAUTIONS (Include drug interactions (synergisms, antagonisms), contraindications, etc.)
17. ANTIDOTE
18.STATUS (Check one)
INVESTIGATIONAL
PHASE I
PHASE II PHASE III
COMMERCIALLY AVAILABLE 0THER (Specify)
19. NAMES OF AUTHORIZED PRESCRIBERS
A. |
|
B. |
|
|
|
C. |
|
D. |
|
|
|
20. SIGNATURE OF RESPONSIBLE OR PRINCIPAL INVESTIGATOR |
DATE |
22. PATIENT IDENTIFICATION (I.D. plate or give name - last, first, middle |
|
|
|
21.APPROVED BY
A.SUBCOMMITTEE ON HUMAN STUDIES
21A. SIGNATURE OF CHAIRPERSON |
|
DATE |
|
|
|
|
|
|
|
|
B. RESEARCH AND DEVELOPMENT COMMITTEE |
|||
|
|
|
|
|
21B. SIGNATURE OF CHAIRPERSON |
|
DATE |
||
|
|
|
|
|
VA FORM |
SUPERSEDES EXISTING STOCK OF VA FORM |
|||
NOV 1989 |
WILL BE USED. |
|||