

Working with PDF files online can be super easy with this PDF tool. You can fill out FEB here within minutes. FormsPal expert team is ceaselessly endeavoring to improve the tool and enable it to be even better for people with its cutting-edge features. Discover an constantly progressive experience today - explore and find new possibilities along the way! With just a few simple steps, you may start your PDF journey:
Step 1: Access the form in our editor by clicking the "Get Form Button" at the top of this webpage.
Step 2: When you start the file editor, you will get the document made ready to be filled in. In addition to filling out different blanks, you may also perform many other things with the form, specifically putting on custom textual content, changing the initial textual content, inserting illustrations or photos, putting your signature on the document, and more.
This PDF form will involve some specific information; to ensure consistency, you need to heed the suggestions directly below:
1. It's important to fill out the FEB properly, thus take care when filling out the segments including these blank fields:
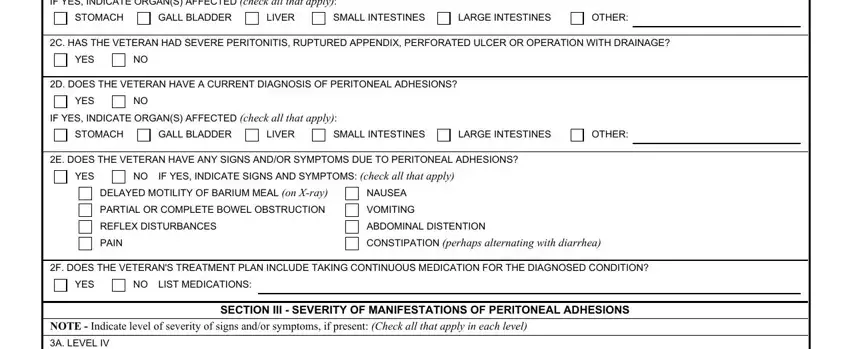
2. After performing the last section, go to the subsequent step and fill in all required particulars in all these blanks - IF YES INDICATE ORGANS AFFECTED, STOMACH, GALL BLADDER, LIVER, SMALL INTESTINES, LARGE INTESTINES, OTHER, C HAS THE VETERAN HAD SEVERE, YES, D DOES THE VETERAN HAVE A CURRENT, YES, IF YES INDICATE ORGANS AFFECTED, STOMACH, GALL BLADDER, and LIVER.
When it comes to OTHER and IF YES INDICATE ORGANS AFFECTED, be sure that you don't make any errors in this section. These could be the key fields in the PDF.
3. The following step is considered fairly straightforward, A LEVEL IV, SEVERE, DEFINITE PARTIAL OBSTRUCTION SHOWN, FREQUENT EPISODES OF SEVERE COLIC, FREQUENT EPISODES OF SEVERE NAUSEA, FREQUENT EPISODES OF SEVERE, PROLONGED EPISODES OF SEVERE COLIC, PROLONGED EPISODES OF SEVERE NAUSEA, PROLONGED EPISODES OF SEVERE, B LEVEL III, MODERATELY SEVERE, PARTIAL OBSTRUCTION MANIFESTED BY, LESS FREQUENT EPISODES OF PAIN, LESS PROLONGED EPISODES OF PAIN, and C LEVEL II - every one of these empty fields needs to be filled in here.
4. It is time to fill out this next segment! In this case you have these A DOES THE VETERAN HAVE ANY SCARS, YES, IF YES ARE ANY OF THE SCARS, YES, NO If Yes also complete VA Form F, B DOES THE VETERAN HAVE ANY OTHER, YES, NO If Yes describe brief summary, HAS THE VETERAN HAD LABORATORY OR, YES, NO If Yes provide type of test or, SECTION V DIAGNOSTIC TESTING, BASED ON YOUR EXAMINATION ANDOR, YES, and NO If Yes describe the impact of form blanks to fill in.
5. Lastly, this final segment is precisely what you need to complete prior to finalizing the form. The blanks you're looking at are the next: REMARKS If any, CERTIFICATION To the best of my, SECTION VIII PHYSICIANS, A PHYSICIANS SIGNATURE, B PHYSICIANS PRINTED NAME, C DATE SIGNED, D PHYSICIANS PHONE AND FAX NUMBER, E PHYSICIANS MEDICAL LICENSE NUMBER, F PHYSICIANS ADDRESS, NOTE VA may request additional, IMPORTANT Physician please fax, VA Regional Office FAX No, NOTE A list of VA Regional Office, and PRIVACY ACT NOTICE VA will not.
Step 3: When you've reviewed the details provided, click "Done" to finalize your document generation. Download your FEB as soon as you join for a 7-day free trial. Easily use the pdf form within your FormsPal account, together with any edits and changes being conveniently kept! With FormsPal, it is simple to fill out forms without needing to worry about personal information leaks or entries being shared. Our protected software helps to ensure that your private information is kept safely.