
Pruritus can be completed in no time. Just use FormsPal PDF tool to perform the job in a timely fashion. Our editor is constantly evolving to grant the very best user experience achievable, and that's thanks to our dedication to constant development and listening closely to customer comments. This is what you would have to do to get going:
Step 1: Click the "Get Form" button above. It is going to open our tool so that you could begin filling out your form.
Step 2: With our online PDF file editor, you are able to accomplish more than simply fill out blank fields. Try all the features and make your documents look sublime with customized text incorporated, or fine-tune the file's original input to perfection - all comes along with an ability to add stunning images and sign the document off.
This form requires specific details; in order to ensure accuracy and reliability, you need to take note of the recommendations further down:
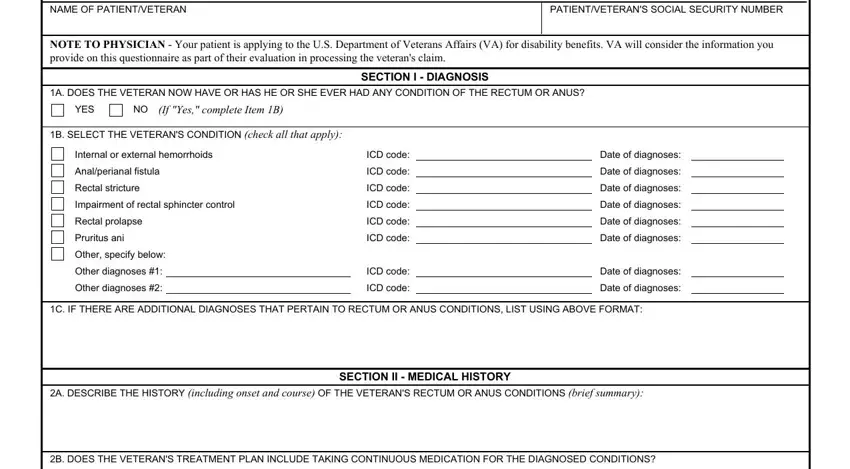
1. The Pruritus needs certain details to be entered. Ensure that the next fields are complete:
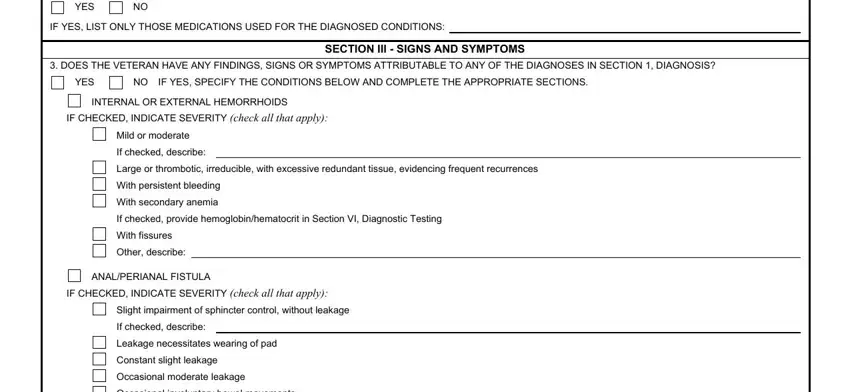
2. Once the previous selection of blanks is filled out, go to type in the suitable information in these: YES, IF YES LIST ONLY THOSE MEDICATIONS, DOES THE VETERAN HAVE ANY, YES, NO IF YES SPECIFY THE CONDITIONS, SECTION III SIGNS AND SYMPTOMS, INTERNAL OR EXTERNAL HEMORRHOIDS, IF CHECKED INDICATE SEVERITY check, Mild or moderate, If checked describe, Large or thrombotic irreducible, With persistent bleeding, With secondary anemia, If checked provide, and With fissures.
3. Completing SECTION III SYMPTOMS OF RECTUM OR, Extensive leakage, Fairly frequent involuntary bowel, Complete loss of sphincter control, Other describe, RECTAL STRICTURE, IF CHECKED INDICATE SEVERITY check, Moderate reduction of lumen, Great reduction of lumen, Moderate constant leakage, Extensive leakage, Requiring colostomy which is, Other describe, IMPAIRMENT OF RECTAL SPHINCTER, and IF CHECKED INDICATE SEVERITY check is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
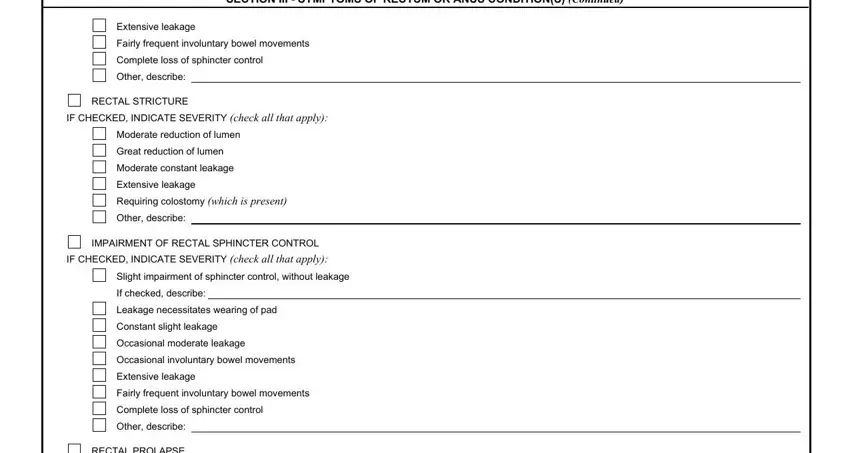
Always be extremely careful when filling out Other describe and Extensive leakage, as this is the part where most users make mistakes.
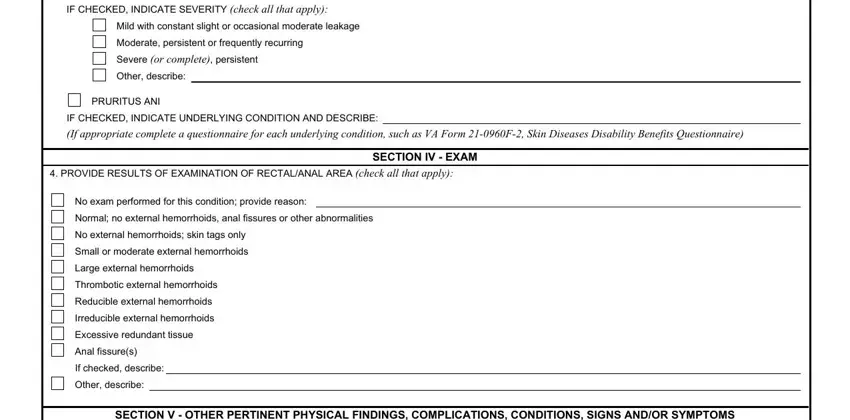
4. The next section needs your information in the subsequent places: IF CHECKED INDICATE SEVERITY check, Mild with constant slight or, Moderate persistent or frequently, Severe or complete persistent, Other describe, PRURITUS ANI, IF CHECKED INDICATE UNDERLYING, If appropriate complete a, PROVIDE RESULTS OF EXAMINATION OF, SECTION IV EXAM, No exam performed for this, Normal no external hemorrhoids, No external hemorrhoids skin tags, Small or moderate external, and Large external hemorrhoids. Make certain to enter all required info to move further.
5. To wrap up your form, this particular part has a couple of extra blank fields. Filling out SECTION I DIAGNOSIS, YES, IF YES ARE ANY OF THE SCARS, YES, If Yes ALSO complete VA Form F, VA FORM H OCT, and Page will certainly conclude the process and you will be done in a snap!

Step 3: Once you've reviewed the information in the blanks, simply click "Done" to finalize your FormsPal process. Get hold of the Pruritus the instant you register here for a 7-day free trial. Instantly gain access to the pdf document from your FormsPal account page, together with any modifications and adjustments automatically synced! FormsPal provides secure document editing devoid of personal data recording or sharing. Rest assured that your details are in good hands here!