
You can work with va form 21 0960m 13 effortlessly with the help of our online tool for PDF editing. To retain our editor on the cutting edge of practicality, we aim to integrate user-oriented capabilities and enhancements on a regular basis. We are at all times thankful for any feedback - help us with revampimg PDF editing. Starting is simple! All that you should do is stick to the next easy steps directly below:
Step 1: Just press the "Get Form Button" in the top section of this webpage to access our pdf editor. Here you will find everything that is necessary to work with your file.
Step 2: Once you start the tool, you will notice the form made ready to be filled in. Besides filling in different fields, you might also do various other things with the Document, such as writing any textual content, modifying the initial text, inserting illustrations or photos, affixing your signature to the form, and more.
Be mindful when completing this pdf. Make certain all mandatory blanks are filled out properly.
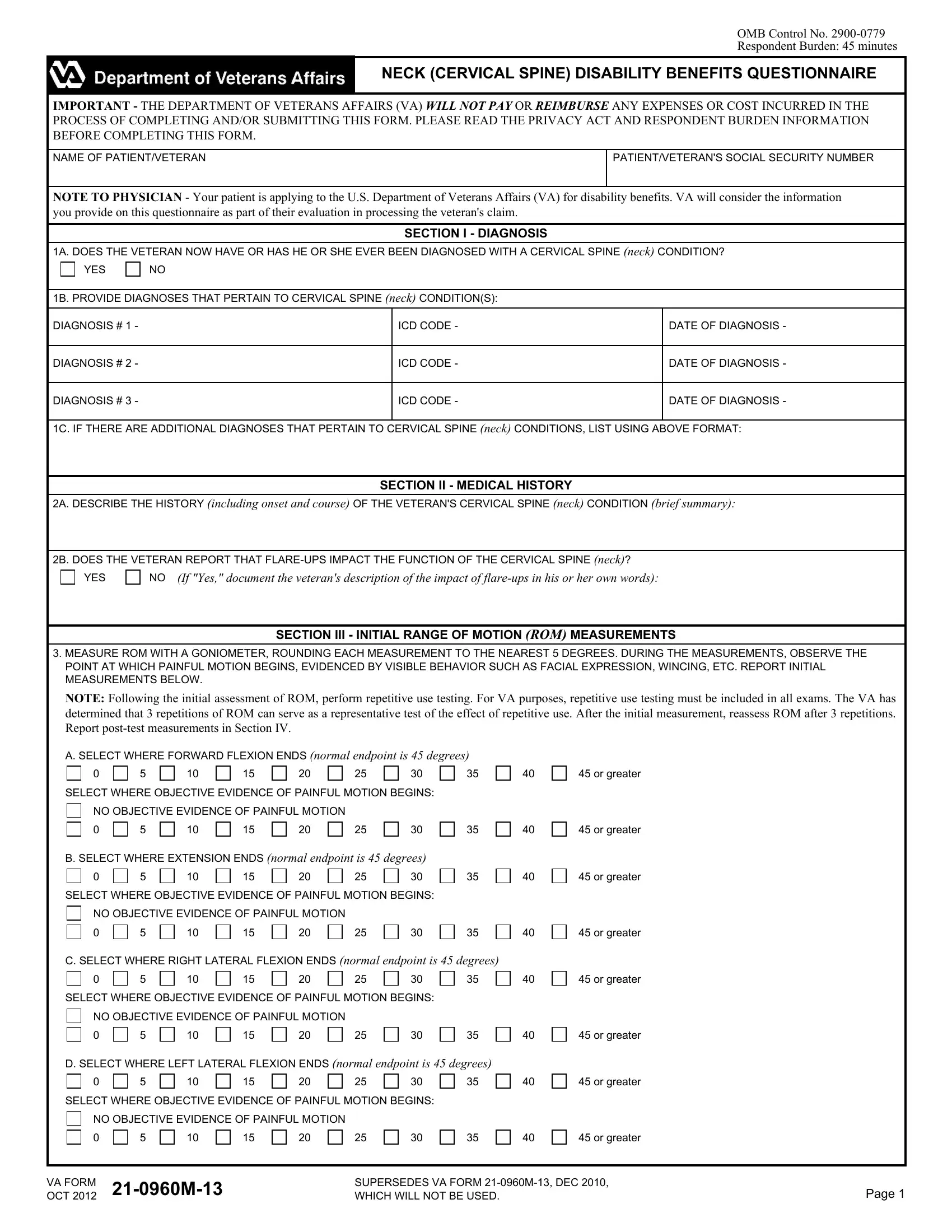
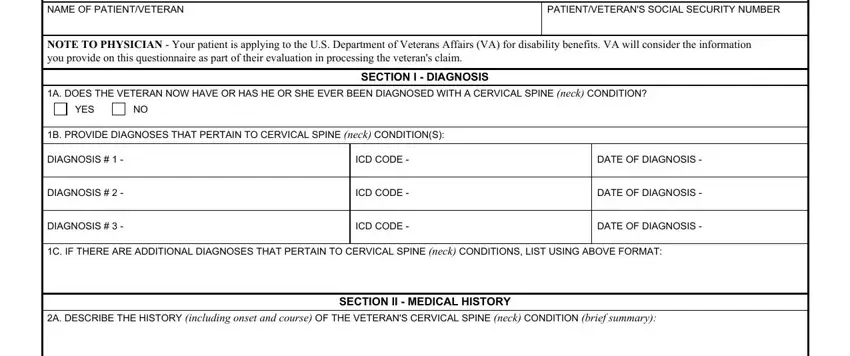
1. Start filling out the va form 21 0960m 13 with a number of major blank fields. Get all of the information you need and make certain there's nothing overlooked!
2. Just after finishing the previous step, go on to the next stage and complete the necessary particulars in these blank fields - B DOES THE VETERAN REPORT THAT, YES, If Yes document the veterans, SECTION III INITIAL RANGE OF, MEASURE ROM WITH A GONIOMETER, POINT AT WHICH PAINFUL MOTION, NOTE Following the initial, A SELECT WHERE FORWARD FLEXION, or greater, SELECT WHERE OBJECTIVE EVIDENCE OF, NO OBJECTIVE EVIDENCE OF PAINFUL, B SELECT WHERE EXTENSION ENDS, SELECT WHERE OBJECTIVE EVIDENCE OF, NO OBJECTIVE EVIDENCE OF PAINFUL, and C SELECT WHERE RIGHT LATERAL.
3. This next part is straightforward - fill out all of the blanks in SELECT WHERE OBJECTIVE EVIDENCE OF, NO OBJECTIVE EVIDENCE OF PAINFUL, or greater, VA FORM OCT M, SUPERSEDES VA FORM M DEC WHICH, and Page in order to complete this part.

4. Your next part will require your information in the following parts: E SELECT WHERE RIGHT LATERAL, or greater, SELECT WHERE OBJECTIVE EVIDENCE OF, NO OBJECTIVE EVIDENCE OF PAINFUL, or greater, F SELECT WHERE LEFT LATERAL, or greater, SELECT WHERE OBJECTIVE EVIDENCE OF, NO OBJECTIVE EVIDENCE OF PAINFUL, or greater, G If ROM does not conform to the, age body habitus neurologic, SECTION IV ROM MEASUREMENTS AFTER, A IS A VETERAN ABLE TO PERFORM, and YES. Always provide all needed information to move onward.
5. When you reach the end of your file, there are actually several more requirements that should be met. Notably, D SELECT WHERE POSTTEST RIGHT, E SELECT WHERE POSTTEST LEFT, F SELECT WHERE POSTTEST RIGHT, G SELECT WHERE POSTTEST LEFT, or greater, or greater, or greater, or greater, SECTION V FUNCTIONAL LOSS, NOTE The following section, A DOES THE VETERAN HAVE ADDITIONAL, YES, B DOES THE VETERAN HAVE ANY, YES, and C IF THE VETERAN HAS FUNCTIONAL must be done.
It is easy to make an error when filling in the NOTE The following section, hence make sure that you reread it before you send it in.
Step 3: Revise what you have inserted in the blanks and hit the "Done" button. Acquire your va form 21 0960m 13 once you join for a free trial. Readily get access to the pdf file within your FormsPal account, along with any edits and adjustments all saved! We don't sell or share the details that you provide when dealing with documents at our site.