
By using the online tool for PDF editing by FormsPal, it is possible to fill in or edit 21 0960 a 1 here and now. Our professional team is constantly endeavoring to expand the editor and ensure it is even easier for clients with its handy features. Take your experience to a higher level with continually improving and exceptional options available today! To get the process started, take these basic steps:
Step 1: Just click the "Get Form Button" in the top section of this page to access our form editing tool. Here you'll find everything that is necessary to work with your document.
Step 2: This editor offers the ability to customize nearly all PDF documents in many different ways. Improve it by adding personalized text, adjust what's originally in the file, and put in a signature - all at your fingertips!
This form will involve some specific information; to ensure correctness, you need to pay attention to the guidelines further on:
1. The 21 0960 a 1 necessitates specific information to be inserted. Make certain the following blank fields are complete:
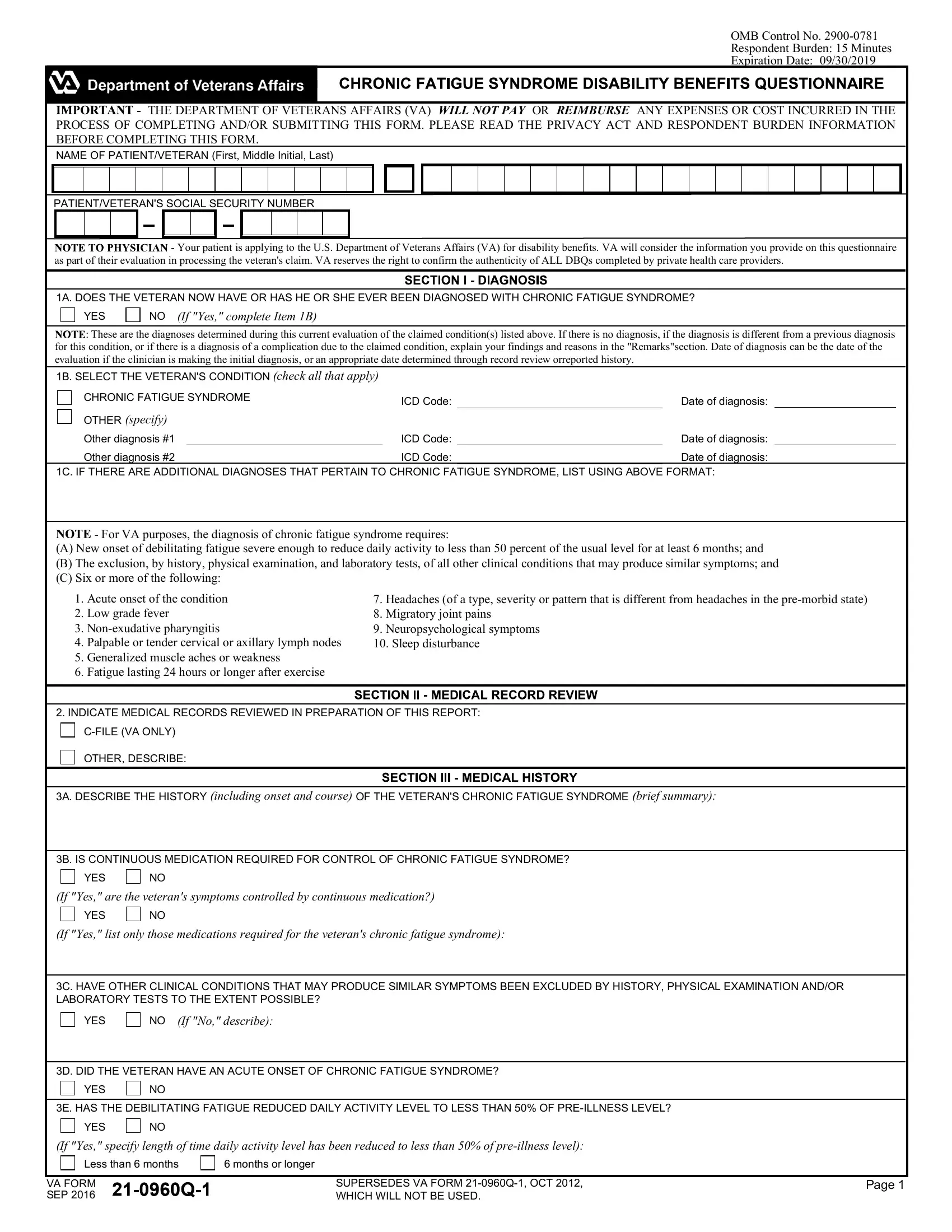
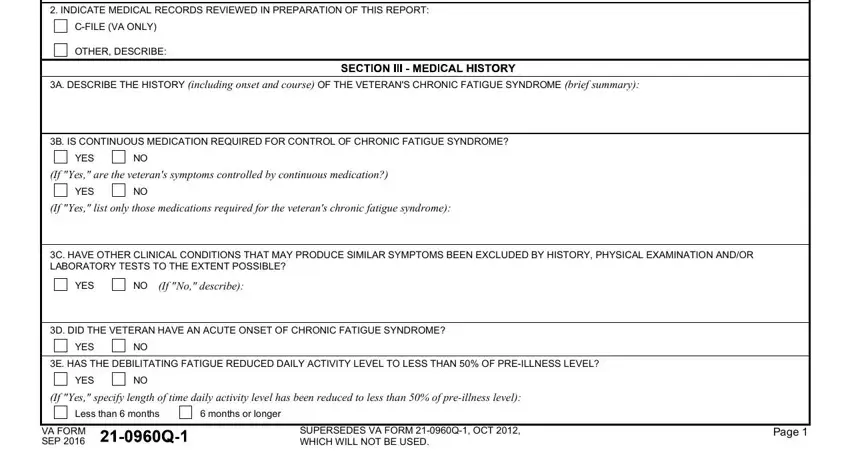
2. The third part is to complete the next few fields: INDICATE MEDICAL RECORDS REVIEWED, CFILE VA ONLY, OTHER DESCRIBE, A DESCRIBE THE HISTORY including, B IS CONTINUOUS MEDICATION, YES, If Yes are the veterans symptoms, YES, If Yes list only those medications, C HAVE OTHER CLINICAL CONDITIONS, YES, If No describe, D DID THE VETERAN HAVE AN ACUTE, YES, and E HAS THE DEBILITATING FATIGUE.
3. This next section is relatively uncomplicated, PATIENTVETERANS SOCIAL SECURITY, A DOES THE VETERAN NOW HAVE OR HAS, YES, If Yes check all that apply, Debilitating fatigue Low grade, Note Describe all checked, and C DOES THE VETERAN NOW HAVE OR HAS - these form fields has to be completed here.
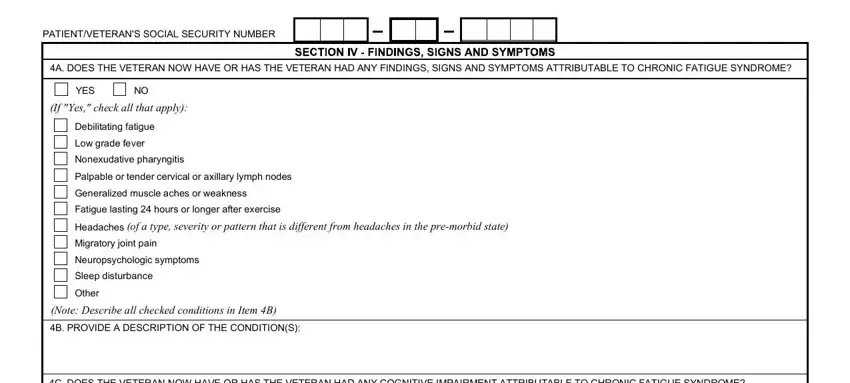
It's easy to make an error while filling in your C DOES THE VETERAN NOW HAVE OR HAS, thus be sure to look again before you'll submit it.
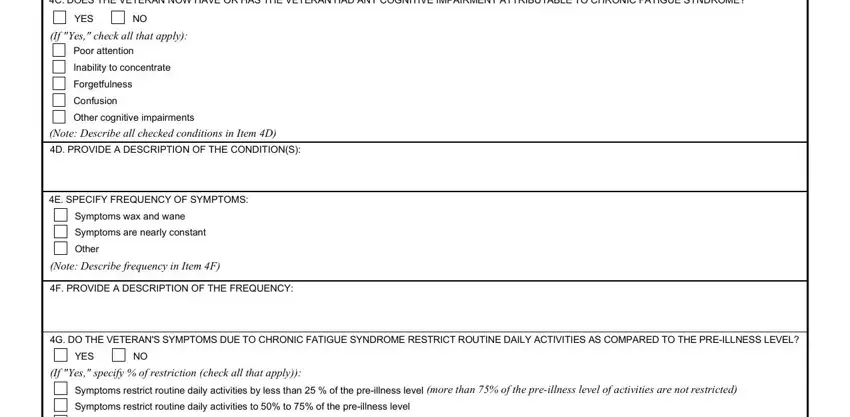
4. The subsequent paragraph requires your details in the subsequent places: C DOES THE VETERAN NOW HAVE OR HAS, YES, If Yes check all that apply, Poor attention Inability to, Note Describe all checked, E SPECIFY FREQUENCY OF SYMPTOMS, Symptoms wax and wane Symptoms are, Note Describe frequency in Item F, F PROVIDE A DESCRIPTION OF THE, G DO THE VETERANS SYMPTOMS DUE TO, YES, If Yes specify of restriction, and Symptoms restrict routine daily. Make certain to fill in all of the needed details to move forward.
5. Now, the following final subsection is precisely what you'll want to finish prior to closing the PDF. The blanks in question are the following: Symptoms restrict routine daily, For VA purposes chronic fatigue, H DO THE VETERANS SYMPTOMS DUE TO, YES, If Yes indicate total duration of, Less than week At least but less, VA FORM Q SEP, and Page.
Step 3: Reread the details you've typed into the blanks and click the "Done" button. Grab your 21 0960 a 1 after you subscribe to a free trial. Quickly use the document within your personal account, with any edits and changes being all saved! At FormsPal, we do our utmost to make sure your details are maintained protected.