We found the best software engineers to set-up our PDF editor. The application will let you create the form 10 2850 document conveniently and won't require too much of your time. This straightforward instruction will let you get going.
Step 1: The very first step requires you to select the orange "Get Form Now" button.
Step 2: Now you may modify the form 10 2850. Feel free to use our multifunctional toolbar to include, delete, and transform the content material of the file.
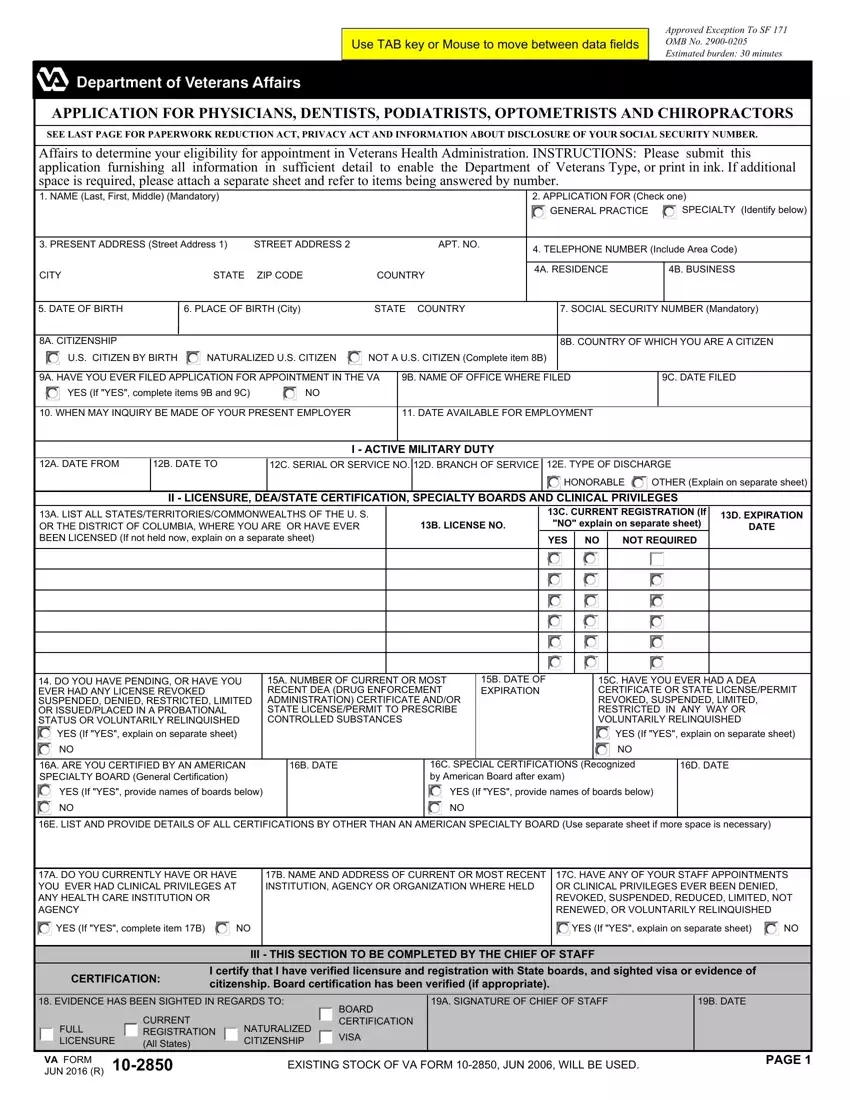
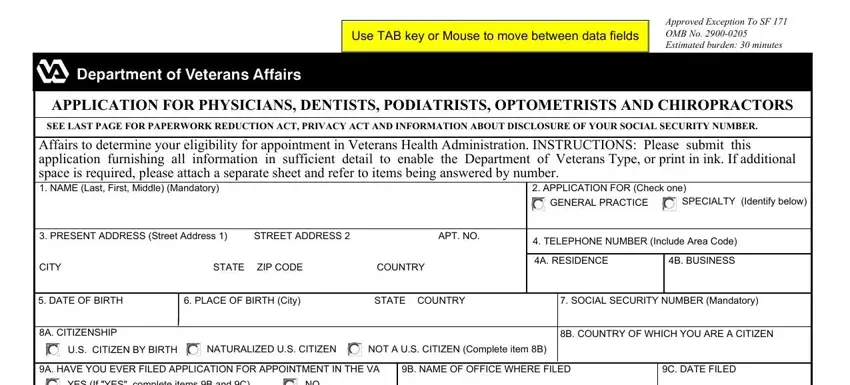
Complete the form 10 2850 PDF and type in the information for each segment:
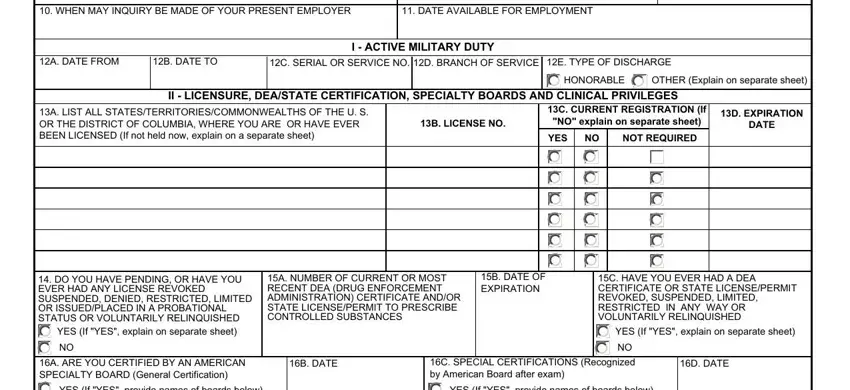
Provide the expected details in the WHEN MAY INQUIRY BE MADE OF YOUR, DATE AVAILABLE FOR EMPLOYMENT, A DATE FROM, B DATE TO, C SERIAL OR SERVICE NO D BRANCH OF, E TYPE OF DISCHARGE, I ACTIVE MILITARY DUTY, II LICENSURE DEASTATE, A LIST ALL, B LICENSE NO, C CURRENT REGISTRATION If NO, D EXPIRATION DATE, YES, NOT REQUIRED, and HONORABLE box.
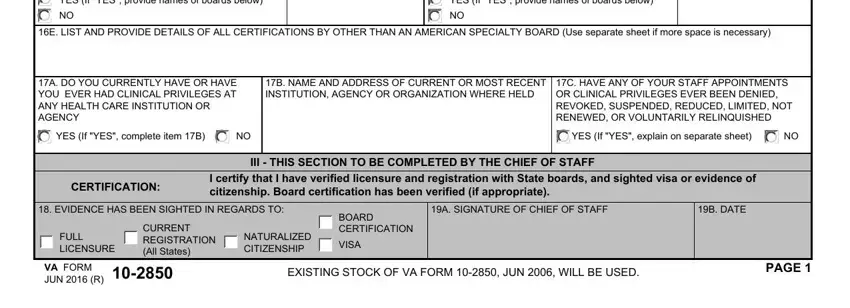
You should identify the key details in the YES If YES provide names of boards, YES If YES provide names of boards, E LIST AND PROVIDE DETAILS OF ALL, A DO YOU CURRENTLY HAVE OR HAVE, YES If YES complete item B, B NAME AND ADDRESS OF CURRENT OR, C HAVE ANY OF YOUR STAFF, YES If YES explain on separate, CERTIFICATION, I certify that I have verified, III THIS SECTION TO BE COMPLETED, EVIDENCE HAS BEEN SIGHTED IN, FULL LICENSURE, CURRENT REGISTRATION All States, and NATURALIZED CITIZENSHIP section.
You'll have to identify the rights and obligations of both sides in field A PRESENT PROFESSIONAL LIABILITY, B DATE COVERAGE BEGAN, C NAMES OF PRIOR CARRIERS, D DATES OF COVERAGE, FROM, V PREPROFESSIONAL EDUCATION, YES, HAS ANY CARRIER EVER CANCELLED, If YES explain on separate sheet, A NAME OF SCHOOL, B ADDRESS City State and ZIP Code, C SUBJECT MAJOR, D YEARS ATTENDED, E GRADUATED YEAR MONTH, and F DEGREE.
Finish by checking these sections and filling them in accordingly: A NAME OF HOSPITAL OR INSTITUTION, B ADDRESS City State and ZIP Code, C SPECIALTY, D PG LEVEL, E COMPLETED YEAR MONTH, F NO OF MONTHS, VIII TEACHING ANDOR RESEARCH, A INSTITUTION, B ADDRESS City State and ZIP Code, C POSITION, D DATE FROM, E DATE TO, A INSTITUTION, B ADDRESS City State and ZIP Code, and C POSITION.
Step 3: Choose the "Done" button. Next, you can transfer your PDF document - download it to your device or send it through email.
Step 4: Generate duplicates of the form - it may help you stay clear of potential complications. And fear not - we don't share or check your details.
