
Handling PDF forms online is actually simple using our PDF tool. Anyone can fill in male reproductive questionnaire here without trouble. Our tool is constantly developing to give the very best user experience possible, and that is thanks to our resolve for continuous development and listening closely to comments from users. Should you be looking to begin, this is what it requires:
Step 1: First of all, access the pdf tool by clicking the "Get Form Button" above on this site.
Step 2: This editor will give you the opportunity to work with the majority of PDF files in various ways. Change it by adding customized text, adjust what's already in the document, and put in a signature - all at your convenience!
Completing this form calls for thoroughness. Make sure every blank field is filled in properly.
1. You will want to complete the male reproductive questionnaire properly, so be mindful while filling out the areas containing all these fields:
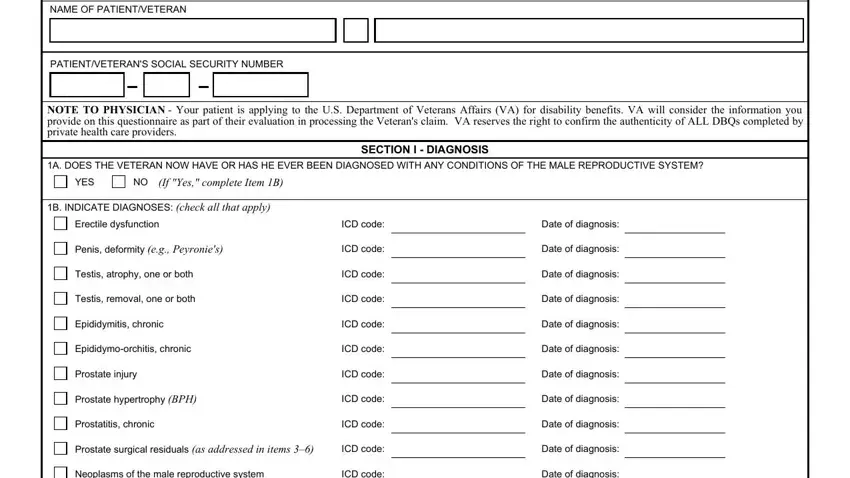
2. Soon after filling out the previous step, go to the next part and complete the necessary details in all these blank fields - Neoplasms of the male reproductive, ICD code, Other male reproductive system, Other diagnosis, Other diagnosis, ICD code, ICD code, Date of diagnosis, Date of diagnosis, Date of diagnosis, C IF THERE ARE ANY ADDITIONAL, A DESCRIBE THE HISTORY including, SECTION II MEDICAL HISTORY, B DOES THE VETERANS TREATMENT PLAN, and YES.
3. In this part, have a look at PATIENTVETERANS SOCIAL SECURITY NO, A DOES THE VETERAN HAVE A VOIDING, YES, If yes complete Items B thru E, If yes provide etiology of voiding, SECTION III VOIDING DYSFUNCTION, B DOES THE VOIDING DYSFUNCTION, YES, Indicate severity check one, Does not require the wearing of, Requires absorbent material which, Requires absorbent material which, Requires absorbent material which, Other describe, and C DOES THE VOIDING DYSFUNCTION. Every one of these need to be filled out with utmost accuracy.
Those who use this document frequently get some things wrong while filling in YES in this area. Be sure you re-examine what you enter here.
4. Completing E DOES THE VOIDING DYSFUNCTION, YES, If yes check all that apply, Hesitancy, If checked is hesitancy marked, YES, Slow or weak stream, If checked is stream markedly slow, YES, Decreased force of stream, If checked is force of stream, YES, Stricture disease requiring, Stricture disease requiring, and Recurrent urinary tract infections is paramount in the fourth step - always spend some time and take a close look at each empty field!
5. As a final point, this last part is precisely what you will need to wrap up before closing the PDF. The fields here include the following: B INDICATE ALL TREATMENT, No treatment, Longterm drug therapy, If checked list medications used, VA FORM J MAY, and Page.
Step 3: After you've looked over the information in the fields, click "Done" to finalize your form at FormsPal. Try a 7-day free trial subscription at FormsPal and acquire direct access to male reproductive questionnaire - download or modify inside your personal account page. We don't share any details that you provide whenever completing documents at our site.