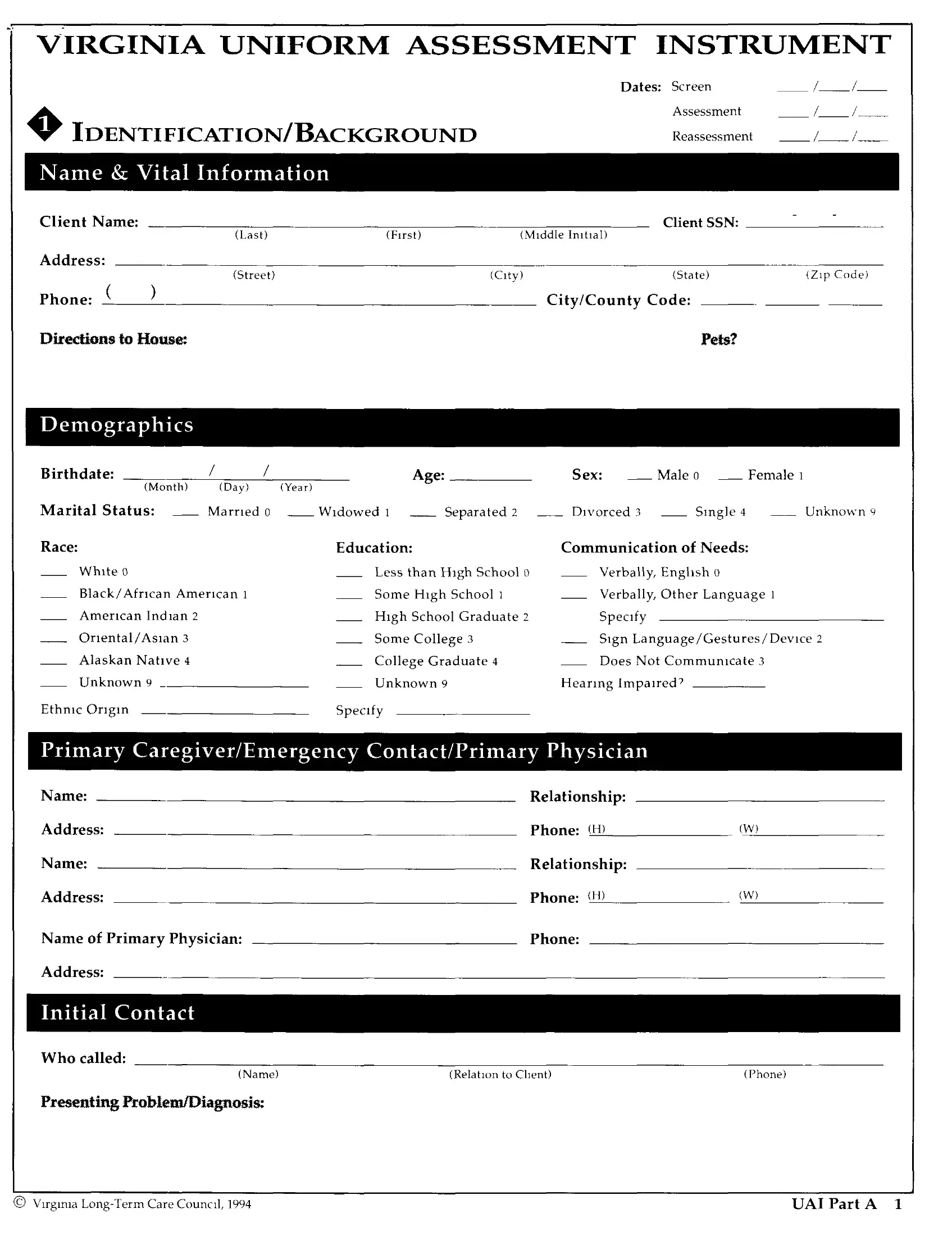
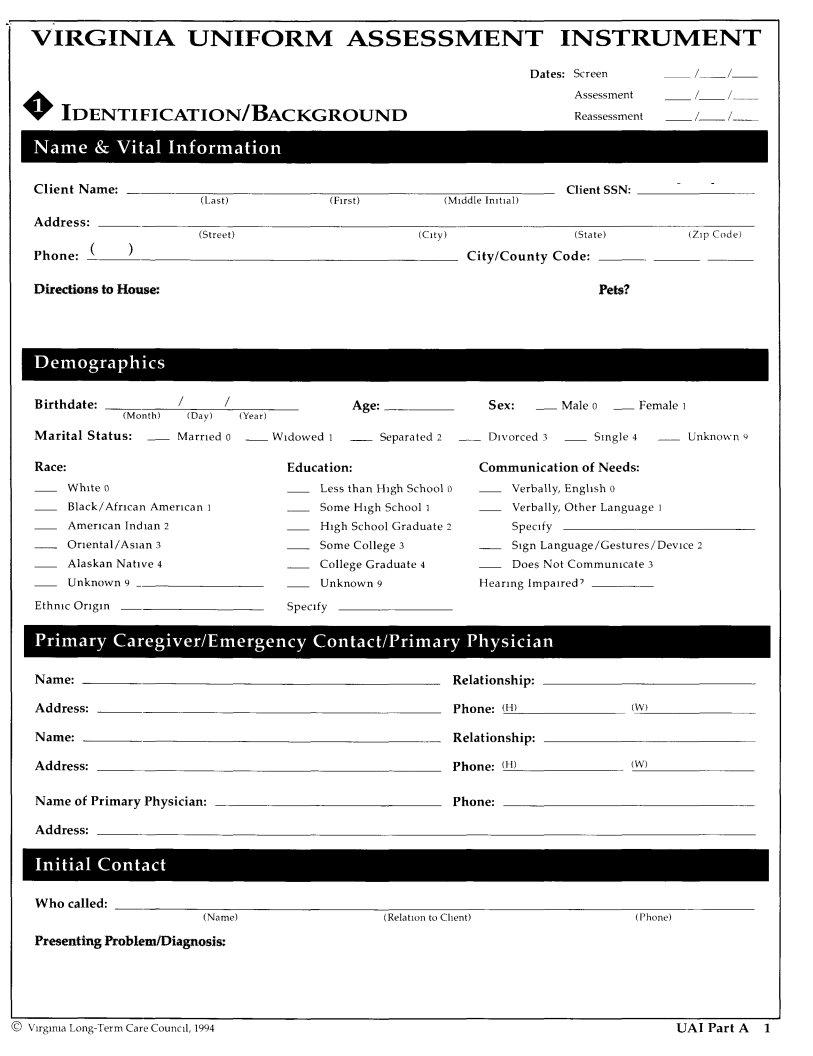
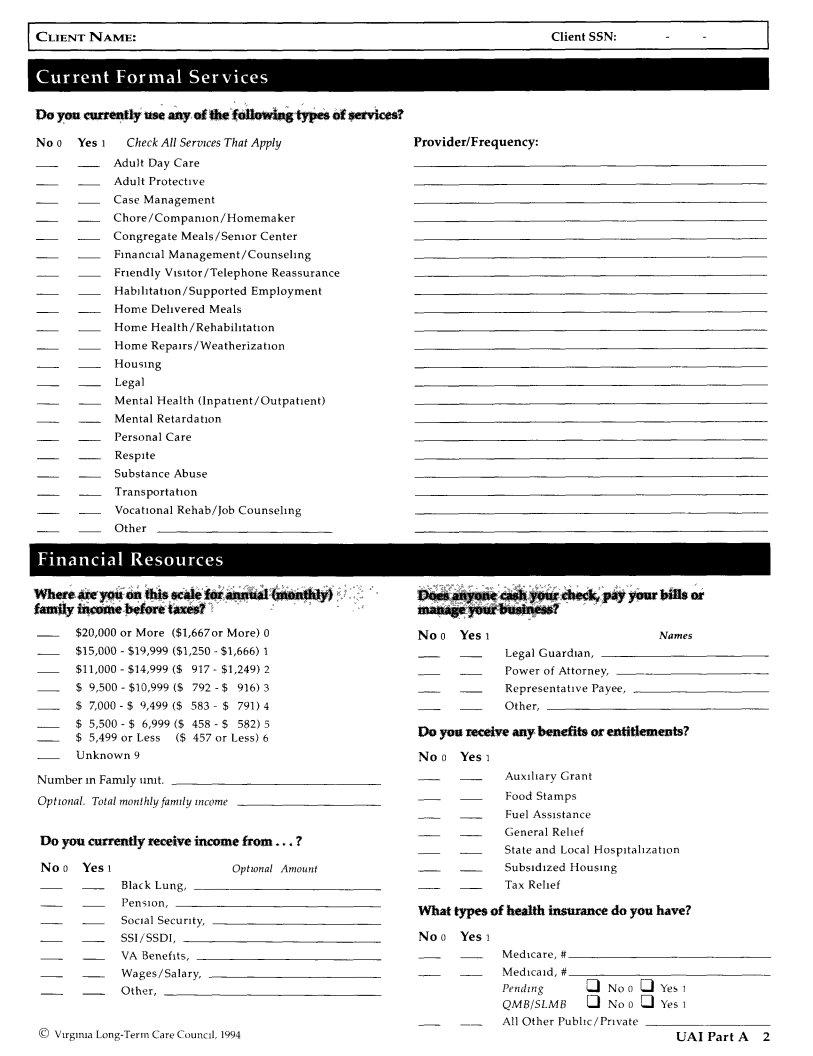
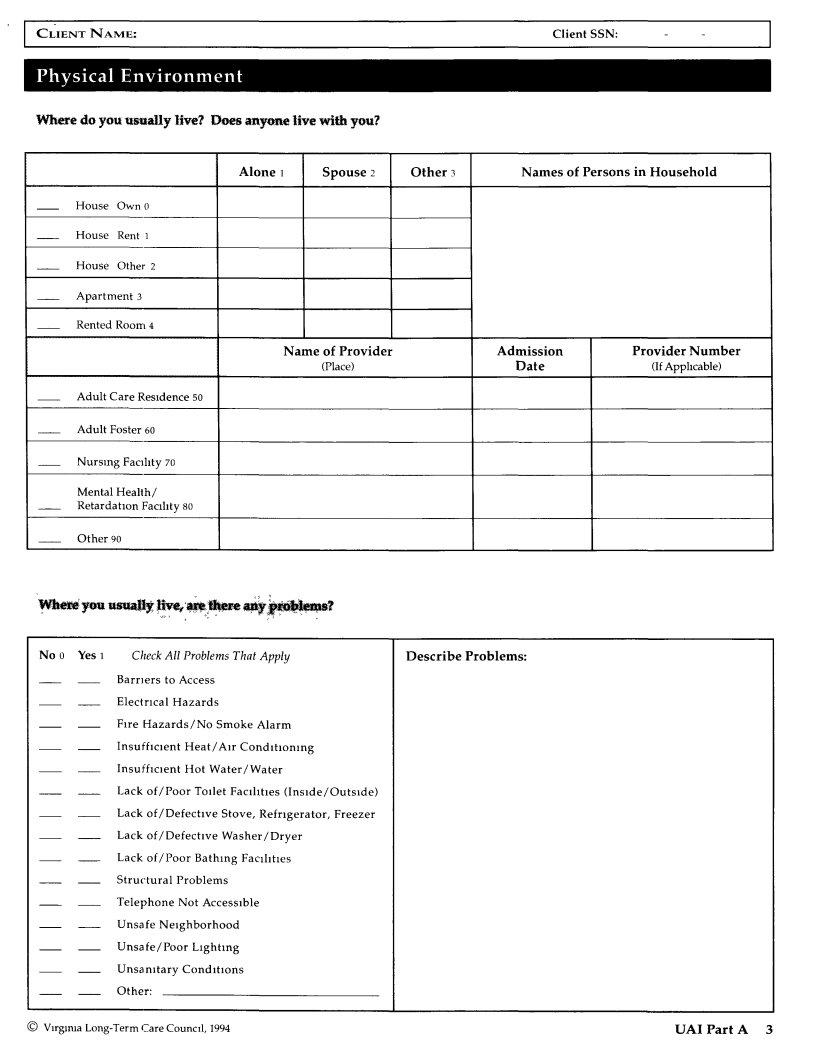
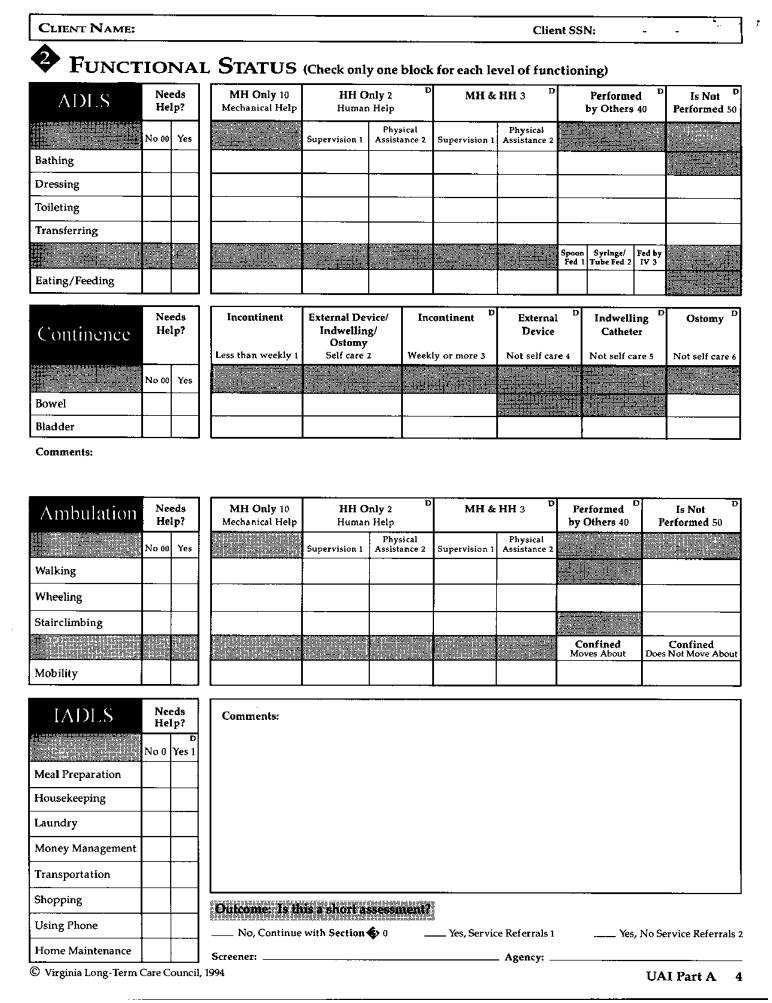
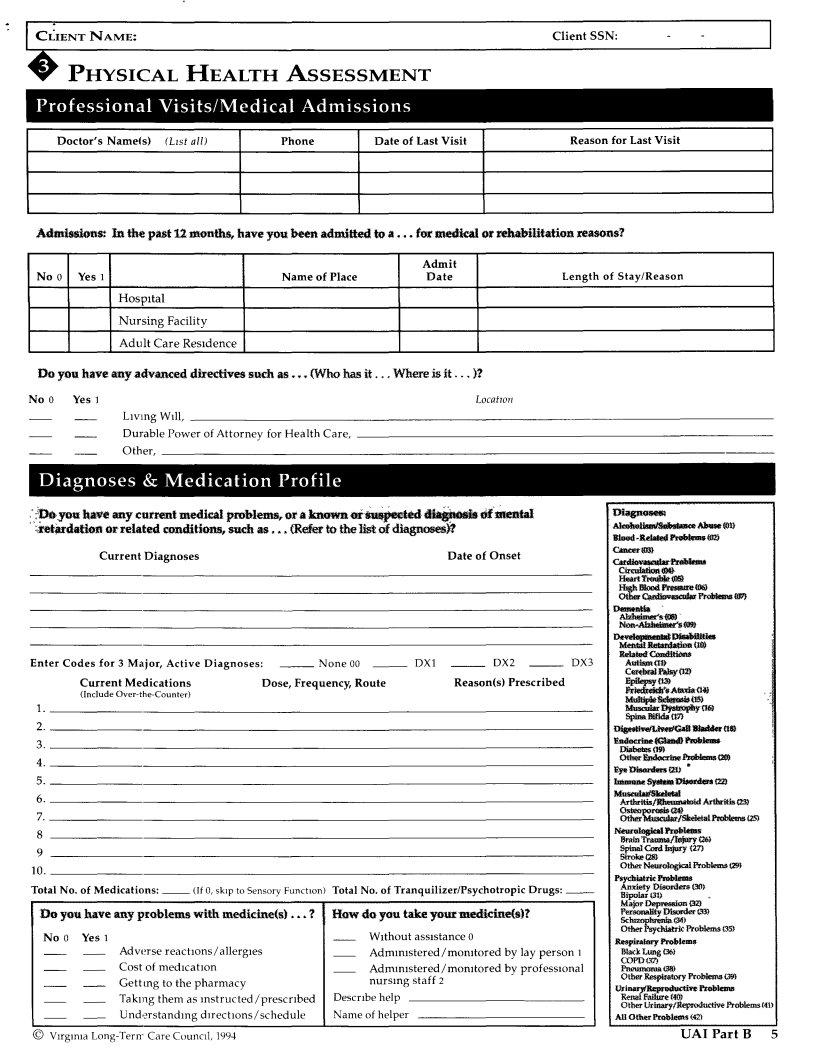
The Virginia Uniform Assessment Instrument, often abbreviated as the VA UAI form, serves as a comprehensive tool designed to assess the needs and background information of individuals requiring long-term care services within Virginia. This detailed document gathers a wide array of vital information, commencing with basic identification and background details such as the client's name, Social Security Number (SSN), address, and other personal identifiers. It delves deeper by inquiring about the client's living arrangements, including whether they live alone or with others, and details regarding their domicile. The form also addresses the physical health of the client, querying about current medical problems, medications, and any hospital admissions within the past 12 months, highlighting the form's thorough nature in assessing an individual's health status. Furthermore, this instrument touches on financial aspects by asking about income sources, types of health insurance, and the client's eligibility for various assistance programs, making it a holistic tool for evaluating the needs of clients in a bid to provide appropriate care and support services. The VA UAI form essentially acts as a critical connector between clients and the services they require, whether those needs are in home care, medical care, or financial assistance, showcasing its role in facilitating long-term care planning and coordination.
| Question | Answer |
|---|---|
| Form Name | Va Uai Form |
| Form Length | 12 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 3 min |
| Other names | virginia uniform assessment instrument, certification uai, what is a uai online, virginia uai form |
VIRGINIA UNIFORM ASSESSMENT INSTRUMENT
IDENTIFICATION/BACKGROUND
Dates: Screen |
/ |
AssessmentReassessment __ /
Client |
Name: |
|
|
Client |
SSN: |
|
|
|
(Last) |
(First) |
(Mlddle ImtlaI) |
|
|
Address: |
|
|
|
|
|
|
|
|
(Street) |
|
(City) |
(State) |
(Zip Code) |
Phone: |
( |
) |
|
City/County |
Code: |
|
Directions |
|
to House: |
|
|
Pets? |
|
Birthdate: |
|
/ |
/ |
|
Age: |
|
|
|
Sex: |
__ |
Male |
0 __ Female |
1 |
(Month) |
(Day) |
|
(Year) |
|
|
|
|
|
|
|
|
|
|
Marital Status: |
__ |
Married |
0 |
__ Widowed 1 |
__ |
Separated |
2 |
Divorced |
3 |
__ |
Single 4 |
Unknown 9 |
|
Race: |
|
|
|
Education: |
|
|
|
Communication of Needs: |
|
||||
White 0 |
|
|
|
Less than High School 0 |
Verbally,Enghsh 0 |
|
|||||||
Black/African |
American 1 |
|
Some |
High |
School 1 |
|
Verbally, |
Other |
Language 1 |
|
|||
American Indian |
2 |
|
High |
School |
Graduate |
2 |
Specify |
|
|
|
|||
Oriental/Asian |
3 |
|
|
Some |
College |
3 |
|
Sign Language/Gestures/Device |
2 |
||||
Alaskan Native 4 |
|
|
College Graduate 4 |
|
Does Not Commumcate 3 |
|
|||||||
Unknown9 |
|
|
|
Unknown9 |
|
|
HearingimpalredP |
|
|
||||
EthnicOrigin |
|
|
|
Specify |
|
|
|
|
|
|
|
|
|
Name: |
Relationship: |
|
Address: |
Phone:(H) |
(W) |
Name: |
Relationship: |
|
Address: |
Phone:(H) |
tW) |
Name of Primary Physician: |
Phone: |
|
Address: |
|
|
Who called:
(Name)(RelahontoChent)(Phone)
Presenting Problem/Diagnosis:
© |
UAl Part A 1 |
I CLIENTNAME: |
ClientSSN: |
- |
No 0 Yes 1 |
CheckAll |
Servzces That Apply |
Provider/Frequency: |
||||
|
Adu]t |
Day |
Care |
|
|
|
|
|
Adult |
Protective |
|
|
|
||
|
Case Management |
|
|
|
|||
|
Chore/Companion/Homemaker |
|
|
||||
|
Congregate |
|
Meals |
/ Senior |
Center |
|
|
|
Financial |
Management/Counseling |
|
||||
|
Friendly |
Visitor/Telephone |
Reassurance |
|
|||
|
Habfiltatlon/Supported |
Employment |
|
||||
|
Home |
Delivered |
Meals |
|
|
||
|
Home |
Health/Rehabilitation |
|
|
|||
|
Home |
Repalrs/Weatherizatlon |
|
||||
|
Housing |
|
|
|
|
|
|
|
Legal |
|
|
|
|
|
|
|
Mental Health (Inpatient/Outpatient) |
|
|||||
|
Mental |
Retardation |
|
|
|
||
|
Personal |
Care |
|
|
|
||
|
Respite |
|
|
|
|
|
|
|
Substance |
|
Abuse |
|
|
|
|
Transportation
Vocational Rehab/Job Counseling
Other
$20,000or More ($1,667orMore)0 |
|
No 0 |
Yes 1 |
|
|
|
|
|
Names |
||||||||
$15,000 - $19,999 ($1,250 - $1,666) 1 |
|
|
Legal |
Guardian, |
|
|
|
||||||||||
$11,000 - $14,999 ($ |
917- |
$1,249) |
2 |
|
|
Power |
of |
Attorney, |
|
|
|||||||
$ 9,500 - $10,999 ($ |
792 |
- $ |
916) |
3 |
|
|
Representative |
Payee, |
|
|
|||||||
$ |
9,499($ |
583- |
$ |
791)4 |
|
|
|
Other, |
|
|
|
|
|
|
|||
$ |
|
6,999($ |
582) |
5 |
|
|
|
|
|
|
|
|
|
||||
$ |
5,499 or |
Less |
($ |
457 |
or |
Less) |
6 |
|
Do your4_q_ve anybenefi_ |
_fifi_? |
|
|
|||||
Unknown9 |
|
|
|
|
|
|
No 0 |
Yes1 |
|
|
|
|
|
|
|||
Numberin Familyunit. |
|
|
|
|
|
|
AuxiliaryGrant |
|
|
||||||||
Optional. |
Total monthly farmly income |
|
|
|
|
Food |
Stamps |
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
Fuel |
Assistance |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
General |
Relief |
|
|
|
||
DO yOU |
currently receive |
income |
from.,. |
? |
|
State |
and |
Local |
Hospltahzatlon |
||||||||
No 0 Yes 1 |
|
|
|
|
|
Optwnal |
Amount |
|
Subsidized |
Housing |
|
|
|||||
|
Black Lung, |
|
|
|
|
|
|
Tax Relief |
|
|
|
|
|||||
|
Pension, |
|
|
|
|
|
V_/hat |
insurance |
do |
you |
have? |
||||||
|
Social |
Security, |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
SSI/SSDI, |
|
|
|
|
|
No 0 |
Yes |
|
|
|
|
|
|
|||
|
VA Benefits, |
|
|
|
|
|
|
Medicare, |
|
# |
|
|
|
||||
|
Wages/Salary, |
|
|
|
|
|
|
Medicaid, |
|
# |
|
|
|
||||
|
Other, |
|
|
|
|
|
|
|
Pending |
|
_ No |
0 _1 |
Yes |
||||
QMB/SLMB |
[] No 0 [] |
Yes |
All Other Public/Private |
|
|
© Virginia |
|
UA1 Part A 2 |
CLIENTNAME: |
ClientSSN: |
- |
Where do you usually live? Does anyone live with you?
Alone 1 |
Spouse 2 |
Other 3 |
Names of Persons in Household |
HouseOwn0
House Rent 1
House Other 2
i
Apartment 3
Rented Room 4
|
|
Name of Provider |
Admission |
Provider Number |
|
|
(Place) |
Date |
(IfApphcable) |
AdultCareResldence50 |
|
I |
||
Adult Foster |
60 |
|
|
|
Nursing |
Facfilty 70 |
|
|
|
Mental |
Health/ |
|
|
|
Retardation |
Facility 80 |
|
|
|
|
|
|
|
I |
Other |
90 |
|
|
l |
|
|
|
||
No 0 Yes l |
Check All Problems That Apply |
Describe |
Problems: |
Barriers to Access
Electrical Hazards
Fire Hazards/No Smoke Alarm
Insufficient Heat/Air Conditioning
Insufficient Hot Water/Water
Lack of/Poor Toilet Facilities (Inside/Outside)
Lack of/Defective Stove, Refrigerator, Freezer
Lack of/Defective Washer/Dryer
Lack of/Poor Bathing Faclhtles
Structural Problems
Telephone Not Accessible
Unsafe Neighborhood
Unsafe/Poor Lighting
Unsanitary Conditions
Other:
© |
UAI Part A 3 |
I CI'.IENTNAME: |
ClientSSN: |
- |
PHYSICAL HEALTH ASSESSMENT
|
|
|
I |
|
Doctor's Name_s) |
(L_st all) |
Phone |
Date of Last Visit |
Reason for Last Visit |
Admissions.- In the past i2 months, have you been admired to a ,.. for medical or rehabfiitation reasons?
|
|
Admit |
|
No 0 Yes 1 |
Name of Place |
Date |
Length of Stay/Reason |
Hospital |
|
|
|
NursingFacility |
|
! |
|
Adult Care Residence |
|
|
|
Do |
you have any advanced directives such as... (Who has it.., Where is it.., |
)? |
No0 |
YesI |
Locatwn |
|
Living Wdl, |
|
|
Durable Power of Attorney for Health Care, |
|
|
Other, |
|
;?_,y(m |
have |
any current medical |
problems, |
or a _or |
_i_tearl |
_i_,_ |
_ |
meltial |
|
|
|
D'_osem |
|
|
|
|||||
_lr_dation |
or related |
conditmns, |
such as,** |
(Refer |
to the |
llst of diagnoses_ |
|
|
|
|
|
: _ |
'__0_ |
!'roMt,m_ |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
slooa |
|
|||
|
|
CurrentDiagnoses |
|
|
|
|
|
DateofOnset |
|
|
|
_ |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cat_1_tar_ulat_ |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C_reulattca_ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
H_a't_nml_ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
i |
|
|
|
|
Enter Codes for |
3 Major, |
Active Diagnoses: |
__ |
None 00 __ |
DX1 |
__ |
DX2 |
__ |
|
DX3 |
|
Au_ismlt_ |
|
|
||||||
|
|
Current Medications |
|
Dose, Frequency, |
Route |
|
Reason(s) Prescribed |
|
|
|
Elvlk'P_i_ |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
_i_Ataltat |
¢f_ |
.: |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
__._ |
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_l_ac, |
|
cal_ |
tt_ |
|
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_ulo_a_na_ |
|
|
||
4. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Er._ |
|
;n) ' |
|
|
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
lmmu_ S_ |
Dl_a*a_*s |
|||
6. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_hat, |
|
tal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Azhkrttlsl |
.Rlmmna_d A.*flu4tis |
||
7. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Osmoporosi_sa0 |
eaaaemsc2_ |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ot_l_luKtaatt_l |
||||
8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N_roIo_i_t_bbmu |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Brain Tra_n_/_ |
126) |
|
|
9 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Stroke_ |
|
|
|
10. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OtherNatr_Pr_lems |
tz_ |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Psychia_rki_al_m |
|
|||
Total |
No. of Medications: |
(If 0, skip to Sensory |
Function) Total |
No. of Tranquilizer/Psychotropic |
Drugs: |
|
|
Anxiety Diaord_rO0)s |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bipolar |
(3D |
., |
|
||
Do |
you |
have any p_oblems |
with |
medicine(s). |
? |
How |
do you take your medicine(s)? |
|
|
|
|
P_r_ |
_m_ |
|
||||||
No 0 |
Yes1 |
|
|
|
|
|
|
W_thoutassistance0 |
|
|
|
|
|
Psyckla feProblemTs35) |
||||||
|
|
|
|
|
|
|
|
|
|
R_pir_ _b_m |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
Adw_'rse reactions/allergies |
|
|
Admm_stered/momtored |
by lay person |
1 |
|
__ |
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COPD_3_ |
|
|
|
|
|
|
Cost of me&cat_on |
|
|
|
Admm_stered/momtored |
by professional |
|
|
P_m) |
|
|
|
||||||
|
|
|
Gettmg |
to the |
pharmacy |
|
|
nursing |
staff 2 |
|
|
|
|
|
|
ot_s__09_ |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ttsri_!m_twav_ l'r_ |
||||
Taking