

Dealing with PDF documents online is actually simple with this PDF tool. You can fill out vanderbilt university release of information here painlessly. To maintain our tool on the forefront of convenience, we strive to integrate user-driven capabilities and enhancements on a regular basis. We're at all times grateful for any feedback - play a vital part in reshaping how you work with PDF files. With just a couple of basic steps, you'll be able to begin your PDF editing:
Step 1: Hit the "Get Form" button at the top of this webpage to access our tool.
Step 2: The tool offers the opportunity to work with your PDF form in a variety of ways. Improve it by writing any text, correct what is originally in the document, and add a signature - all at your fingertips!
Filling out this document requires focus on details. Make sure all mandatory areas are completed properly.
1. You will need to fill out the vanderbilt university release of information accurately, so be mindful while working with the areas including these specific blank fields:
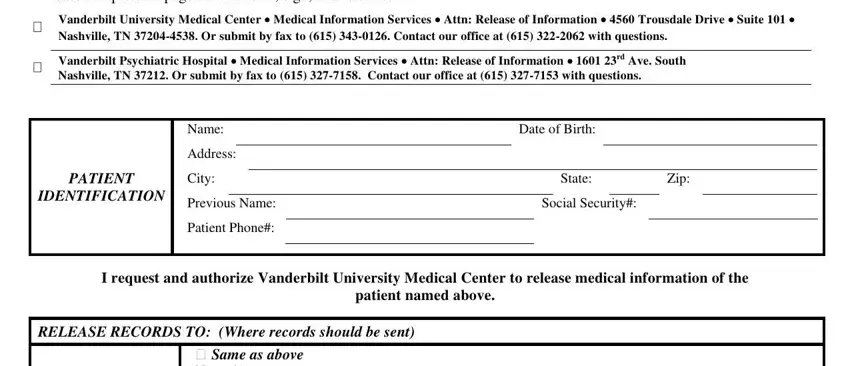
2. Just after this part is filled out, proceed to type in the applicable details in all these - Please complete all pages of this, Vanderbilt University Medical, Vanderbilt Psychiatric Hospital, Name, Address, PATIENT, City, IDENTIFICATION, Previous Name, Patient Phone, Date of Birth, State, Zip, Social Security, and I request and authorize Vanderbilt.
Those who use this form often make mistakes when filling out City in this area. Be sure you go over whatever you enter right here.
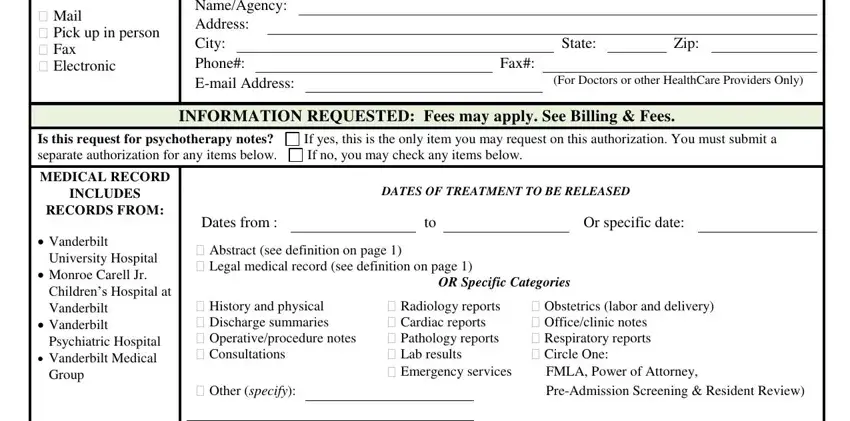
3. Completing Mail Pick up in person Fax, Same as above, NameAgency Address City Phone, State, Zip, Fax, For Doctors or other HealthCare, INFORMATION REQUESTED Fees may, Is this request for psychotherapy, If yes this is the only item you, MEDICAL RECORD, INCLUDES, RECORDS FROM, Vanderbilt, and University Hospital is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. Filling out OTHER, DEPARTMENT, The information to be released, cid Payment Records, specify, Specific Date, and Page of MC Rev is essential in the next step - you should definitely don't rush and fill in each and every blank area!

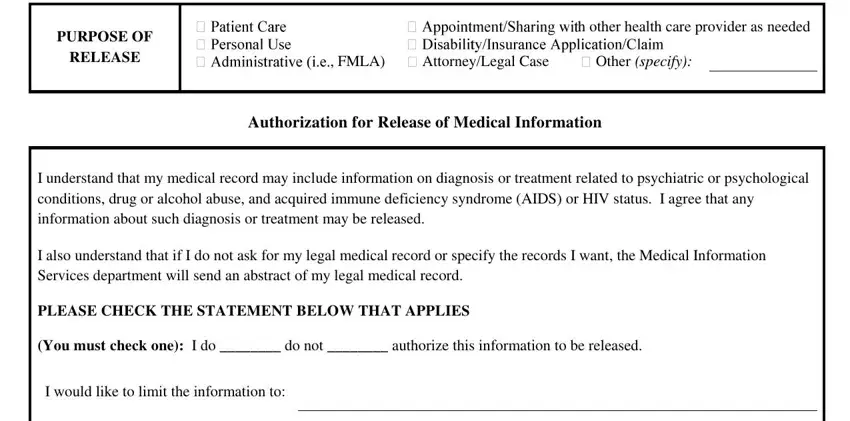
5. The last point to complete this document is crucial. Ensure you fill in the displayed form fields, such as PURPOSE OF, RELEASE, FMLA, AttorneyLegal Case, h other health care provider as, Other specify, Authorization for Release of, I understand that my medical, and I would like to limit the, before finalizing. Neglecting to do it may generate a flawed and probably incorrect document!
Step 3: Right after proofreading the fields, press "Done" and you are done and dusted! Obtain the vanderbilt university release of information the instant you subscribe to a 7-day free trial. Quickly view the pdf file from your FormsPal account, together with any edits and changes being all synced! FormsPal is devoted to the confidentiality of our users; we make sure that all personal data entered into our system stays secure.