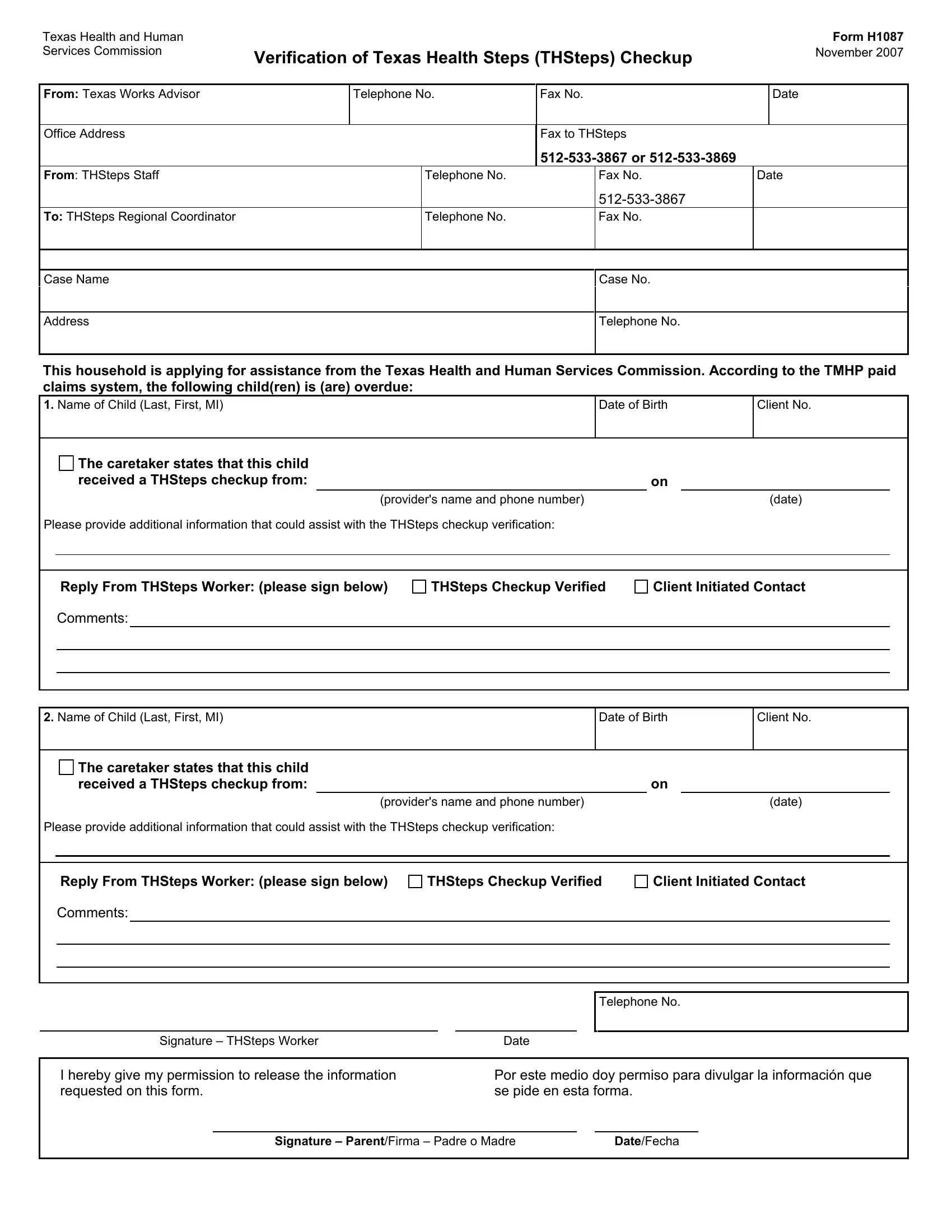
In navigating the intricacies of health care and assistance programs, the Verification of Texas Health Steps (THSteps) Checkup Form (H1087, November 2007) unfolds as a crucial document for families interacting with the Texas Health and Human Services Commission. This form serves as a bridge between households applying for assistance and the THSteps regional coordinators, ensuring that children in these households receive the necessary health checkups as part of the program's requirements. It meticulously records the child's name, date of birth, and client number, followed by details of their latest THSteps checkup, including the provider's name and contact information. Furthermore, the form is designed to gather additional data that might aid in the verification process of the THSteps checkup. On a procedural level, it involves communication lines between Texas Works advisors, THSteps staff, and the regional coordinator, encapsulated in telephone and fax numbers for efficient information exchange. At its core, the form is also a consent document, where parents or guardians authorize the release of pertinent health checkup information, highlighting the collaborative effort between families and health services to ensure children's well-being. This synthesis of logistical coordination and focused care underscores the form's role in facilitating a streamlined approach to health services verification within Texas' public assistance frameworks.
| Question | Answer |
|---|---|
| Form Name | Verification Thsteps Checkup Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | verification checkup online, h1087, verification health checkup, tx steps thsteps |
Texas Health and Human Services Commission
Verification of Texas Health Steps (THSteps) Checkup
Form H1087
November 2007
From: Texas Works Advisor
Telephone No.
Fax No.
Date
Office Address
Fax to THSteps
From: THSteps Staff |
Telephone No. |
Fax No. |
Date |
|
|
|
To: THSteps Regional Coordinator |
Telephone No. |
Fax No. |
Case Name
Case No.
Address
Telephone No.
This household is applying for assistance from the Texas Health and Human Services Commission. According to the TMHP paid claims system, the following child(ren) is (are) overdue:
1. Name of Child (Last, First, MI) |
Date of Birth |
Client No. |
|
|
|
|
|
The caretaker states that this child |
|
|
|
|
|
|
|
|
|
||
|
|
received a THSteps checkup from: |
|
|
|
|
|
on |
|
|
|
||
|
|
|
|
(provider's name and phone number) |
|
|
(date) |
|
|||||
Please provide additional information that could assist with the THSteps checkup verification: |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Reply From THSteps Worker: (please sign below) |
THSteps Checkup Verified |
Client Initiated Contact |
|
||||||||
|
|
Comments: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|||||
2. Name of Child (Last, First, MI) |
|
|
|
|
Date of Birth |
|
Client No. |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
The caretaker states that this child |
|
|
|
|
|
|
|
|
|
||
|
|
received a THSteps checkup from: |
|
|
|
|
|
on |
|
|
|
||
|
|
|
|
(provider's name and phone number) |
|
|
(date) |
|
|||||
Please provide additional information that could assist with the THSteps checkup verification: |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
||||
|
|
Reply From THSteps Worker: (please sign below) |
THSteps Checkup Verified |
Client Initiated Contact |
|
||||||||
|
|
Comments: |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telephone No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature – THSteps Worker |
|
|
Date |
|
|
|
|
|||
I hereby give my permission to release the information requested on this form.
Por este medio doy permiso para divulgar la información que se pide en esta forma.
Signature – Parent/Firma – Padre o Madre |
Date/Fecha |