We've applied the hard work of the best programmers to create the PDF editor you are going to apply. The software allows you to prepare the print vshl sports physical form without trouble and don’t waste time. All you need to undertake is comply with these straightforward guidelines.
Step 1: Hit the orange "Get Form Now" button on the webpage.
Step 2: Now you will be on your file edit page. You'll be able to add, alter, highlight, check, cross, include or remove areas or text.
The next few sections are what you are going to fill in to have the prepared PDF form.
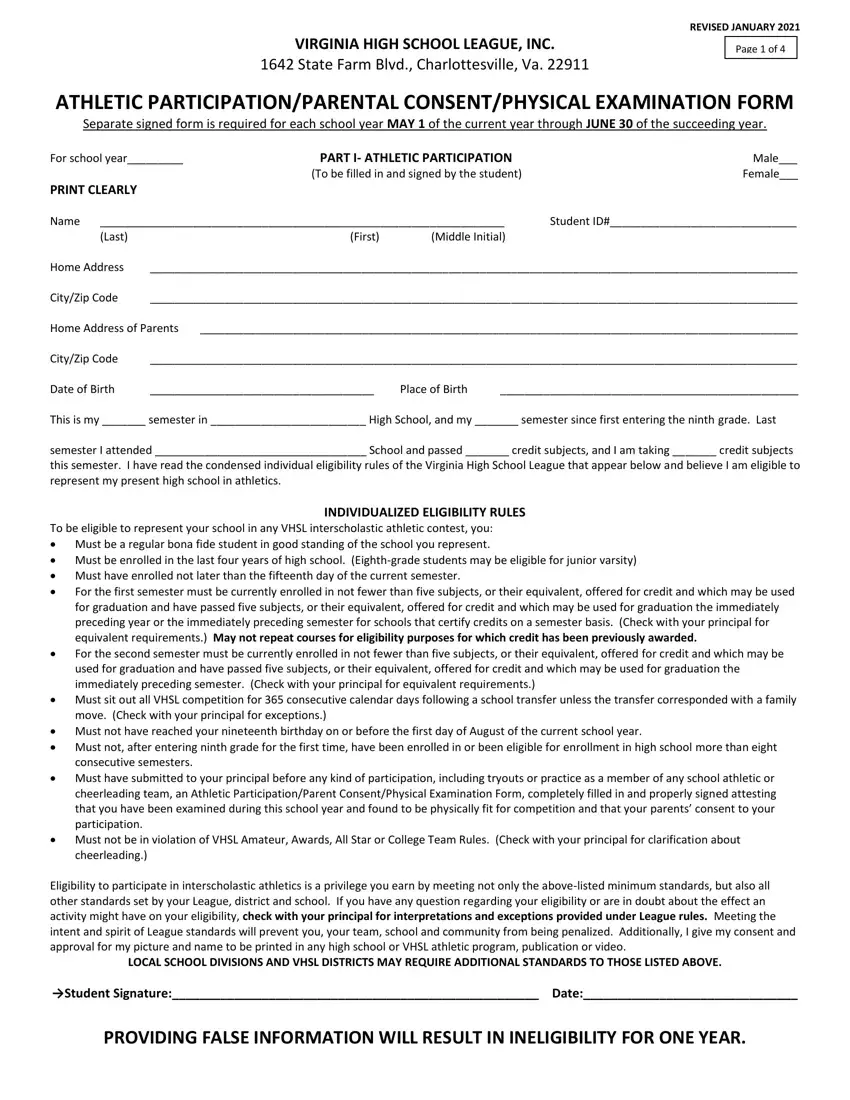
In the Eligibility to participate in, LOCAL SCHOOL DIVISIONS AND VHSL, Student Signature Date, and PROVIDING FALSE INFORMATION WILL box, jot down your details.

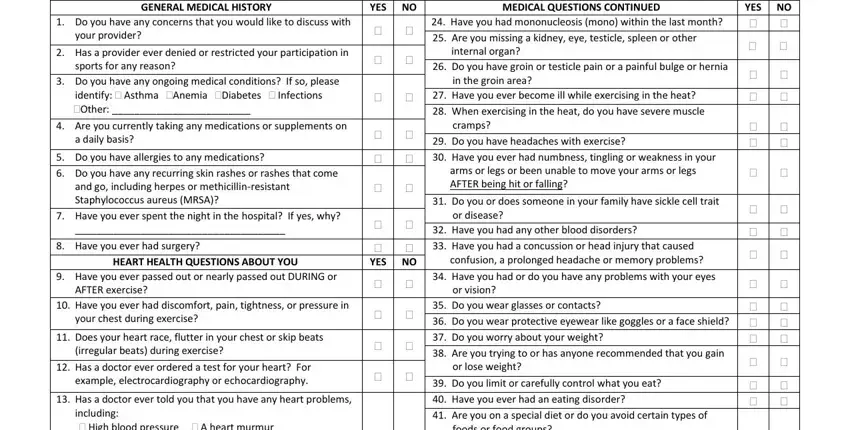
The program will require you to include specific vital info to automatically submit the section GENERAL MEDICAL HISTORY Do you, your provider, Has a provider ever denied or, sports for any reason, Do you have any ongoing medical, Other Are you currently taking, a daily basis, Do you have allergies to any, and go including herpes or, Have you ever spent the night in, Have you ever had surgery, HEART HEALTH QUESTIONS ABOUT YOU, Have you ever passed out or, AFTER exercise, and Have you ever had discomfort pain.
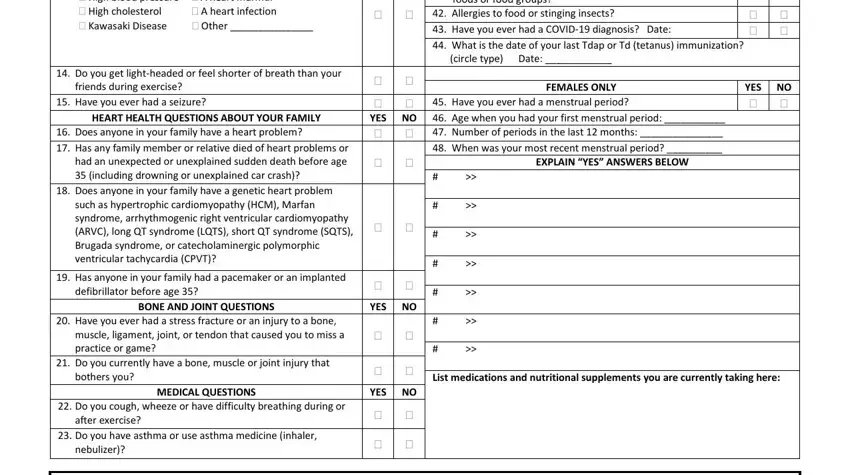
Inside the field High blood pressure A heart, Do you get lightheaded or feel, friends during exercise Have you, HEART HEALTH QUESTIONS ABOUT YOUR, Does anyone in your family have a, Does anyone in your family have a, Has anyone in your family had a, defibrillator before age, BONE AND JOINT QUESTIONS, Have you ever had a stress, muscle ligament joint or tendon, Do you currently have a bone, bothers you, MEDICAL QUESTIONS Do you cough, and after exercise, identify the rights and responsibilities of the sides.
End by analyzing the next fields and filling them out as needed: ParentGuardian Signature Date.

Step 3: Hit the button "Done". Your PDF document is available to be exported. You will be able obtain it to your laptop or email it.
Step 4: Make duplicates of the document. This will save you from upcoming troubles. We don't check or publish your details, therefore you can be confident it is safe.
