COMMONWEALTH OF VIRGINIA
Department of Health
Dear Heath Care Professional:
The Virginia Women, Infants, and Children (WIC) Program promotes breastfeeding as the optimal feeding method for infants. For those infants who do consume formula, Similac Advance and Similac Soy Isomil are offered. A contract with Abbott Nutrition for these formulas provides a special price that allows the WIC program to serve more participants in Virginia. Due to this contract, Virginia WIC is unable to provide standard infant formulas which are made by other manufacturers (ex. Mead Johnson (Enfamil), Nestle (Gerber Good Start), or generic/store brands).
Medical conditions may require the use of special formulas for infants and the use of special formula, nutritionals, and/or modified food benefits for children and women. If a Virginia WIC participant in your care requires one of these items, a special food prescription can be issued after the completion of this WIC-395 request form. All participants receiving a special food prescription remain eligible to receive age/category appropriate WIC supplemental foods as medically indicated.
A new WIC-395 request form is required at each WIC subsequent certification appointment or at the end of the duration indicated, whichever occurs first. In addition, a new request form will also be required when any changes to the food prescription are requested.
The current Virginia WIC Formulary of approved Formulas/Nutritionals can be found at:
http://www.vdh.virginia.gov/wic-participants/food-packages-and-infant-formula/
Further details about issuance of Ready To Feed (RTF) formula can be found at:
http://www.vdh.virginia.gov/content/uploads/sites/42/2017/01/FDS-03.2-C.pdf
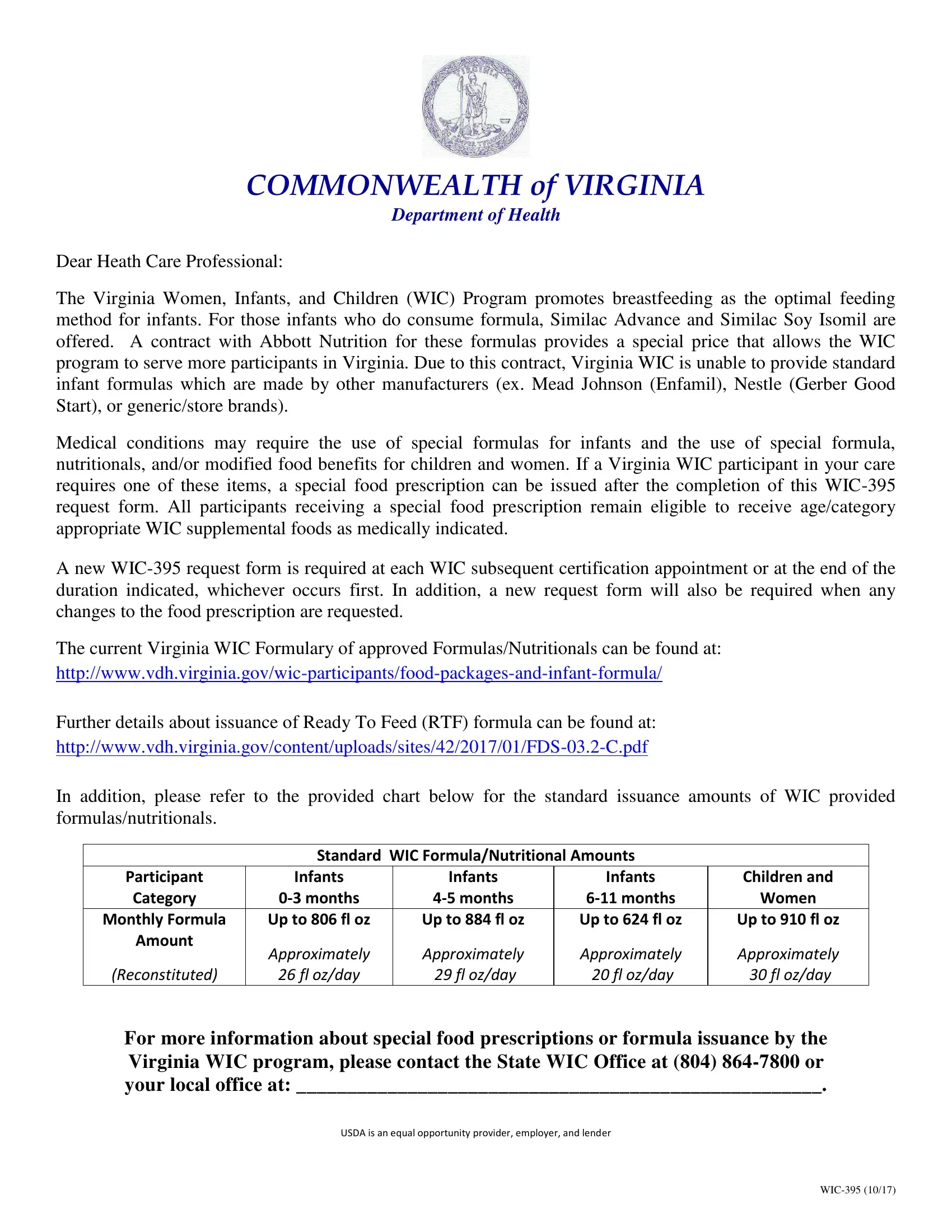
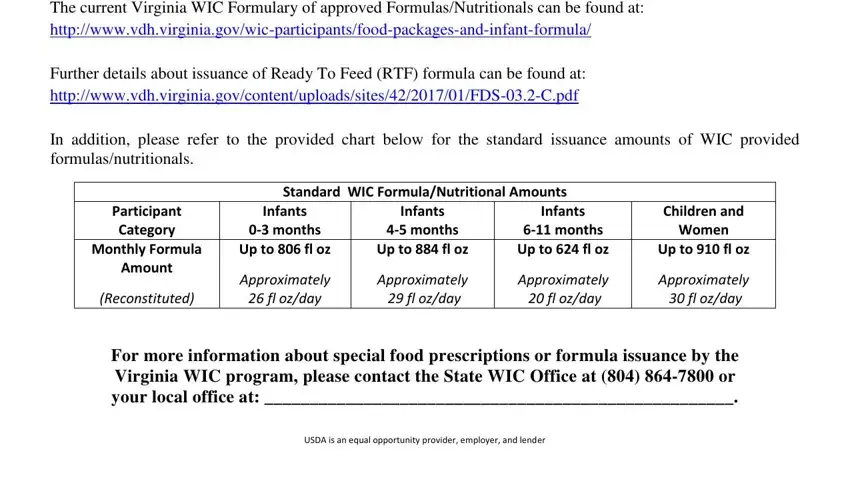
In addition, please refer to the provided chart below for the standard issuance amounts of WIC provided formulas/nutritionals.
Standard WIC Formula/Nutritional Amounts
Participant |
Infants |
Infants |
Infants |
Children and |
Category |
0-3 months |
4-5 months |
6-11 months |
Women |
Monthly Formula |
Up to 806 fl oz |
Up to 884 fl oz |
Up to 624 fl oz |
Up to 910 fl oz |
Amount |
Approximately |
Approximately |
Approximately |
Approximately |
|
(Reconstituted) |
26 fl oz/day |
29 fl oz/day |
20 fl oz/day |
30 fl oz/day |
For more information about special food prescriptions or formula issuance by the Virginia WIC program, please contact the State WIC Office at (804) 864-7800 or your local office at: ____________________________________________________.
USDA is an equal opportunity provider, employer, and lender
WIC-395 (10/17)
Virginia Request
for Special Food Prescription
Prescription is subject to approval and provision based on Virginia WIC policy and procedure.
A. Patient Information
Participant’s Name: |
|
|
Date of Birth: |
|
|
|
Parent/Caregiver’s First and Last Name: |
|
|
|
|
|
B. Current Anthropometric Data |
|
|
|
|
|
|
Weight: |
Length/Height: |
Hgb/Hct: |
Date Assessed: |
|
|
|
|
For intolerances to Similac Advance and/or Similac Soy Isomil due to lactose sensitivity, excessive spit-up, or digestive issues, the following 19 kcal/oz contract infant formulas are available:
C. Alternative Routine Infant Formulas
Similac Sensitive Powder |
Similac Spit-up Powder |
Similac Total Comfort Powder |
Similac Sensitive RTF* |
Similac Spit-up RTF* |
*RTF products require additional justiication and issuance is subject WIC Policy |
If none of the above formulas are appropriate for the participant or if a food prescription modiication is required, please complete the following:
D. Exempt Infant Formulas/Nutritionals
Product Name: _________________________________________________________________________________________
|
|
|
|
Form: Powder |
Concentrate |
RTF* *RTF products require additional justiication and issuance is subject WIC Policy. |
Diagnosis: _____________________________________________ |
ICD Code: _________________________________ |
Symptoms such as colic, constipation, spitting-up, gas, and/or formula intolerance will NOT be accepted. WIC will not provide formula to enhance nutrient intake or manage body weight without underlying medical condition.
Calories Per Ounce: |
Standard Dilution |
OR |
____________ kcal/oz |
Ounces Per Day: |
Standard WIC Amount (Infants Only) |
OR |
_____________ oz* |
*Amounts above the standard WIC maximum are only allowable for participants who meet both Medicaid Coverage and Diagnosis Criteria
E. WIC Supplemental Foods
Issue Full Provision of Age-Appropriate Foods |
Issue NO WIC Supplemental Foods, Provide Formula/Nutritional ONLY |
Issue Supplemental Foods with the Modiications Below:
Infants
Provide formula only due to inability to consume solids
Omit Infant Cereal
Omit Infant Fruits Vegetables
Omit Infant Meats
Children and Women
Provide Infant Pureed |
Provide Whole Milk, |
Provide 2% Milk, |
Fruits/Vegetables |
ICD Code Required: |
ICD Code Required: |
(Formula Use Required) |
________________ |
________________ |
Omit Peanut Butter |
Omit Milk/Cheese/Yogurt |
Omit Whole Grains |
Omit Beans |
Omit Eggs |
Omit Fruits/Vegetables |
Omit Breakfast Cereal |
Omit Juice |
Omit Tuna/Salmon |
F. Length of Use
|
Duration of Certiication, up to 1 year |
OR |
______________ months |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
G. Health Care Provider’s Information (print or stamp) |
|
|
“WIC USE ONLY” |
|
Provider Name: |
|
|
|
|
|
|
Family ID #: |
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CPA Signature: |
|
|
|
Phone: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fax: |
|
|
|
|
|
|
CPA Name: |
|
|
|
|
|
|
|
|
|
Date: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of Health Care Professional authorized |
Date |
|
|
|
|
|
|
|
|
|
to write medical prescriptions under State law. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
USDA is an equal opportunity provider, employer, and lender. |
WIC 395 ( Rev. 10/17) |