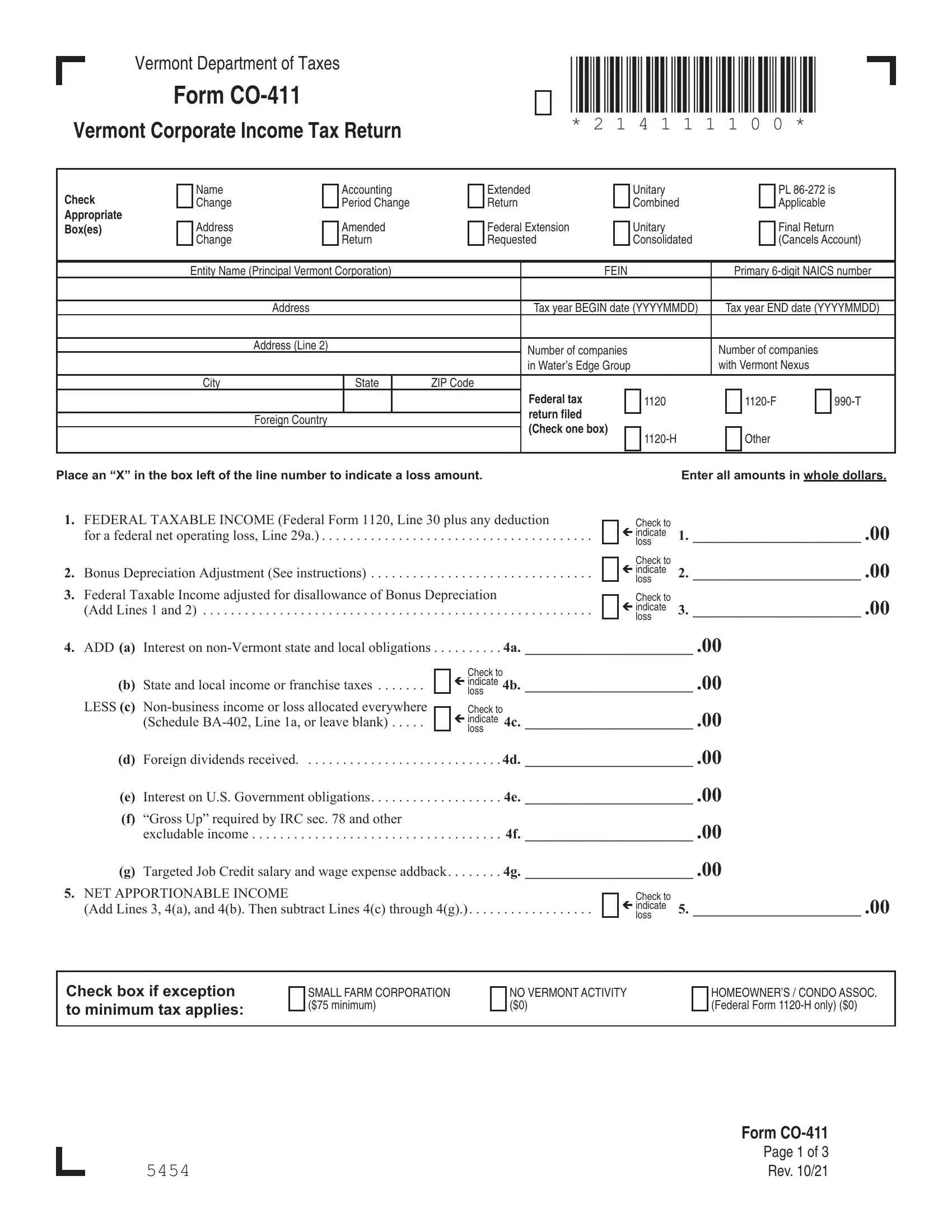
When it comes to corporate taxation in Vermont, navigating the complexities requires a comprehensive understanding of the necessary forms and their implications, especially the Vermont Corporate Income Tax Return, better known as Form CO-411. This form serves as a critical tool for corporations to declare their income tax to the Vermont Department of Taxes. Among its features, Form CO-411 encompasses various sections that cater to different aspects of the corporation's financial activities over the fiscal year, such as federal taxable income adjustments, bonus depreciation, interest on non-Vermont obligations, and credits for taxes overpaid. Additionally, it addresses the intricate tax computation schedules based on Vermont net income and gross receipts, elucidating the minimum tax requirements and calculated tax due. It is structured to also account for payment details, including estimated payments, extensions, and overpayments. Significantly, it allows for adjustments related to Vermont's apportionable and allocable income, ensuring corporations accurately reflect income attributable to the state. Furthermore, unique provisions cater to entities like small farm corporations or those with no Vermont activity, underlining the state's consideration for varying corporate circumstances. On the administrative side, Form CO-411 mandates a declaration from an officer or authorized agent of the corporation, asserting the accuracy and completeness of the return, an essential step in reinforcing the accountability and integrity of the tax filing process. Thus, Form CO-411 encapsulates the critical facets of Vermont's approach to corporate income taxation, providing a structured yet adaptable framework for corporations to comply with state tax laws.
| Question | Answer |
|---|---|
| Form Name | Vt Form Co 411 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | Corporate Income Tax - Vermont Department of Taxes |
