
Using the online PDF editor by FormsPal, you can fill out or alter w 35 form right here. To maintain our editor on the forefront of convenience, we aim to put into action user-oriented capabilities and enhancements regularly. We are routinely happy to receive suggestions - join us in reshaping PDF editing. It merely requires a few simple steps:
Step 1: First, open the editor by clicking the "Get Form Button" in the top section of this page.
Step 2: Using our advanced PDF editing tool, it's possible to do more than merely fill out blanks. Try all of the functions and make your documents look perfect with customized text put in, or tweak the file's original content to perfection - all comes along with the capability to incorporate your personal images and sign the document off.
It is easy to complete the document with our practical tutorial! This is what you have to do:
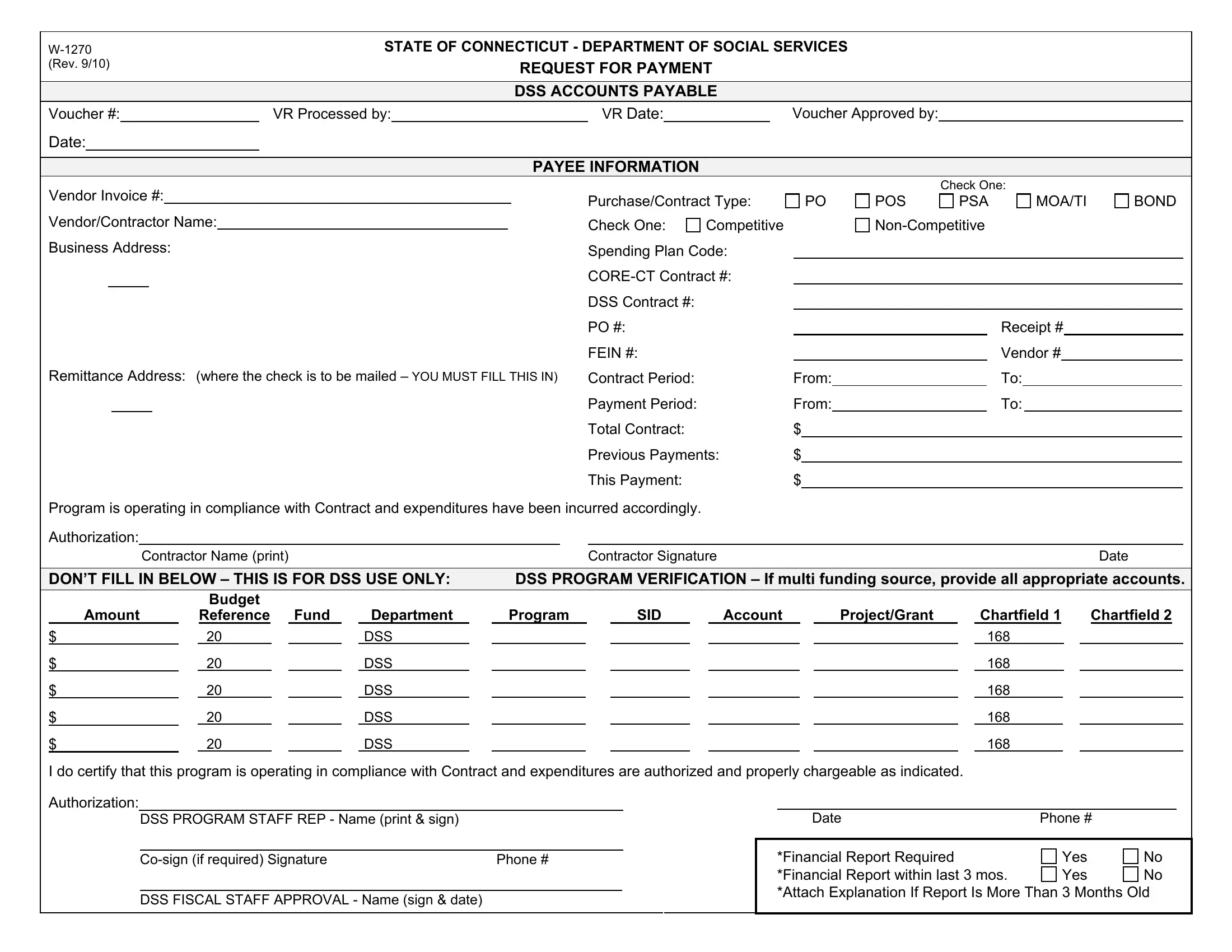
1. Start completing your w 35 form with a group of essential fields. Note all of the necessary information and make certain absolutely nothing is missed!
Step 3: Reread everything you've entered into the blank fields and press the "Done" button. Join FormsPal today and immediately use w 35 form, set for downloading. All modifications made by you are preserved , meaning you can customize the file at a later time if required. At FormsPal, we do our utmost to be certain that all of your details are kept secure.